© 2021 American Dental Association All Rights Reserved. July 2021
Making the Case for Dental Coverage for
Adults in All State Medicaid Programs
Author: Marko Vujicic, Ph.D.; Chelsea Fosse, D.M.D., M.P.H.; Colin
Reusch, M.P.A.; Melissa Burroughs
Introduction
Oral health is essential for overall health and wellness. Oral health is linked with systemic
health conditions and diseases as well as employment opportunities, economic stability, and
social connectedness. One cannot be healthy without a healthy mouth. Yet millions of adults
in America – particularly low-income adults – cannot afford the oral health care they need to
stay healthy, eat, work, socialize, and live pain free. Part of this disparity is driven by gaps in
dental coverage in federal and state policy, particularly dental coverage for adults enrolled in
Medicaid.
As the nation recovers from the COVID-19 pandemic and economic downturn, oral health
coverage is a critical gap in our health care system. For adults who rely on Medicaid, being
able to afford oral health care could be the key to recovering their health or getting a new
job. Yet millions of adults are left without oral health coverage, exacerbating health
inequities. Notably, the people most likely to get sick and lose jobs during the pandemic are
This Research Brief was written
in a partnership between the
ADA Health Policy Institute
(HPI) and Families USA and
Community Catalyst.
The Health Policy Institute is a
thought leader and trusted
source for policy knowledge on
critical issues affecting the U.S.
dental care system. HPI strives
to generate, synthesize, and
disseminate innovative research
for policymakers, oral health
advocates, and dental care
providers.
Community Catalyst is a
consumer health advocacy
organization that seeks to
engage policymakers and other
stakeholders to increase access
and affordability of care through
policy reform.
Families USA is a leading non-
partisan research organization
that provides public health policy
analysis with specific focus on
health care value, health equity,
coverage, and consumer
experience.
Contact the Health Policy
Institute for more information on
products and services at
call 312.440.2928.
Key Messages
Oral health is essential for overall health. Providing adult dental coverage through
Medicaid improves access to and utilization of dental care among low-income adults and
has the power to reduce racial disparities, advance health equity, and lower medical care
costs.
We estimate the cost of implementing extensive dental coverage for adults in all state
Medicaid programs that do not provide such coverage. We estimate increased spending
on dental care as well as medical care cost savings stemming from improved oral health.
Federal and state policymakers have various levers to promote oral health equity across
the nation, including designating dental services as a mandatory benefit category for
adults, establishing a baseline of comprehensiveness for adult dental services in
Medicaid, and bolstering state budgets to ensure adequate funding for successful
implementation.

2
also the people who face the biggest barriers to oral
health. People of color, tribal communities, older
adults, and people with disabilities are among those
who would most benefit from improved oral health
coverage in Medicaid.
In this brief, we review data on barriers to dental care
for low-income adults and the current landscape of
dental coverage for Medicaid-enrolled adults. The data
convincingly show that providing comprehensive dental
coverage for Medicaid-enrolled adults is a major driver
of access to dental care and improved oral health. We
then estimate the fiscal impact of implementing
comprehensive dental coverage for adults in the 28
state Medicaid programs that currently do not provide
such coverage. Our analysis includes estimates of how
many more adults would seek dental care and the
associated dental care costs as well as medical care
cost savings stemming from improved oral health for
those with chronic conditions like diabetes and heart
disease. We also discuss federal policy options to
ensure that all states offer adequate adult dental
coverage in Medicaid that could reduce cost barriers
and improve access to dental care for adults across
the United States.
Financial Barriers to Dental Care by
Income, Age, and Race
Dental care has the highest level of financial barriers
compared to any other health care service.
1
Financial
factors such as lack of insurance and cost being too
high are much more limiting to dental care access than
non-financial factors (e.g., fear of dentist, difficulty
finding an appointment time).
2
This is true for all age
groups and income levels. But the data clearly show
that out of any age group and income group, low-
income adults face the most significant cost barriers to
dental care.
Figure 1 summarizes the latest available data on cost
barriers to dental care. Within any particular income
group, adults consistently face higher cost barriers to
dental care than children or seniors. Children have, by
far, the lowest levels of cost barriers to dental care.
Further, within any particular age group, there is a
significant income gradient in cost barriers to dental
care. Low-income adults face the most significant cost
barriers to dental care out of any age and income
group.

3
Figure 1: Prevalence of Cost Barriers to Dental Care by Age and Income Level
Source: Health Policy Institute analysis of National Health Interview Survey data for 2019. Note: Percentages indicate those who
needed dental care but did not obtain it in the past 12 months due to cost. FPL: federal poverty level.
Financial barriers to dental care for low-income adults
have consequences. Low-income adults are least likely
to access dental care, including basic preventive
services.
3
Low-income adults are more likely than their
higher income peers to experience dental pain, to
report a poor overall condition of their mouth and teeth,
and to find life in general to be less satisfying due to
the condition of their mouth and teeth.
4
Further, poor
oral health also has economic consequences for low-
income adults. Research indicates that nearly 30
percent of low-income adults in the U.S. indicate that
the condition of their mouth and teeth limits their ability
to interview for a job.
4
There are also racial and ethnic disparities in oral
health care access that are important to highlight.
Black and Hispanic adults are more likely to face cost
barriers to dental care than White adults, and this gap
has been increasing over time.
5
Among children, cost
barriers to dental care have been narrowing across all
racial and ethnic categories. Black and Hispanic adults
are also less likely to have had a dental visit compared
to their White and Asian peers. Racial and ethnic
disparities in dental care utilization among children
have been decreasing.
6
6%
8%
2%
15%
24%
5%
26%
32%
6%
0% 5% 10% 15% 20% 25% 30% 35%
Seniors (Age 65+)
Adults (Age 19-64)
Children (Age 2-18)
Low-Income (<133% FPL) Middle-Income (133%-399% FPL) High-Income (400%+ FPL)

4
The Impact of Medicaid Adult Dental
Coverage on Access to Care, Health
Care Costs, and Employability
There is a clear link between Medicaid policy on dental
coverage for adults and cost barriers to dental care,
dental care utilization, oral health status, and
employability. A recent study concluded that when
adults gain dental coverage through Medicaid, they
report improved oral health and employability.
7
These
outcomes were most pronounced among Black
Medicaid enrollees and those who had gone without
dental coverage for more than a year, suggesting that
dental coverage has the potential to reduce income
and race-based inequities in the oral health care
delivery system. Studies show that providing dental
coverage to adults in Medicaid programs significantly
increases access to and utilization of dental care.
8
There are spillover effects for children, as children who
reside in states that provide Medicaid adult dental
coverage to their parents are more likely to have had a
dental visit in the past year and less likely to have
deferred dental care.
9
There are economic benefits to adult dental coverage
in Medicaid. Among Medicaid-enrolled adults in states
that do not provide dental coverage to adults in their
Medicaid program, 60 percent reported that the
appearance of their mouth and teeth affects their ability
to interview for a job.
10
For those in states with dental
coverage for adults, it was much lower, at 35 percent.
10
More broadly, improved oral health could broaden
employment prospects and promote economic activity
in the community.
11
,
12
,
13
Expanded dental coverage can reduce overall medical
costs. Studies have repeatedly shown that dental
coverage significantly reduces costly emergency
department visits for dental conditions.
14
,
15
These cost
savings are realized by diverting care from hospital
emergency departments to more cost-effective settings
like a dental office or community health center. This
diversion can also lead to better oral health outcomes
because patients will get more clinically appropriate
treatment for dental conditions by dental professionals.
There is also emerging evidence that increased access
to dental care can lead to lower medical care costs
among patients who are pregnant or who have chronic
conditions such as diabetes and heart disease.
16
,
17
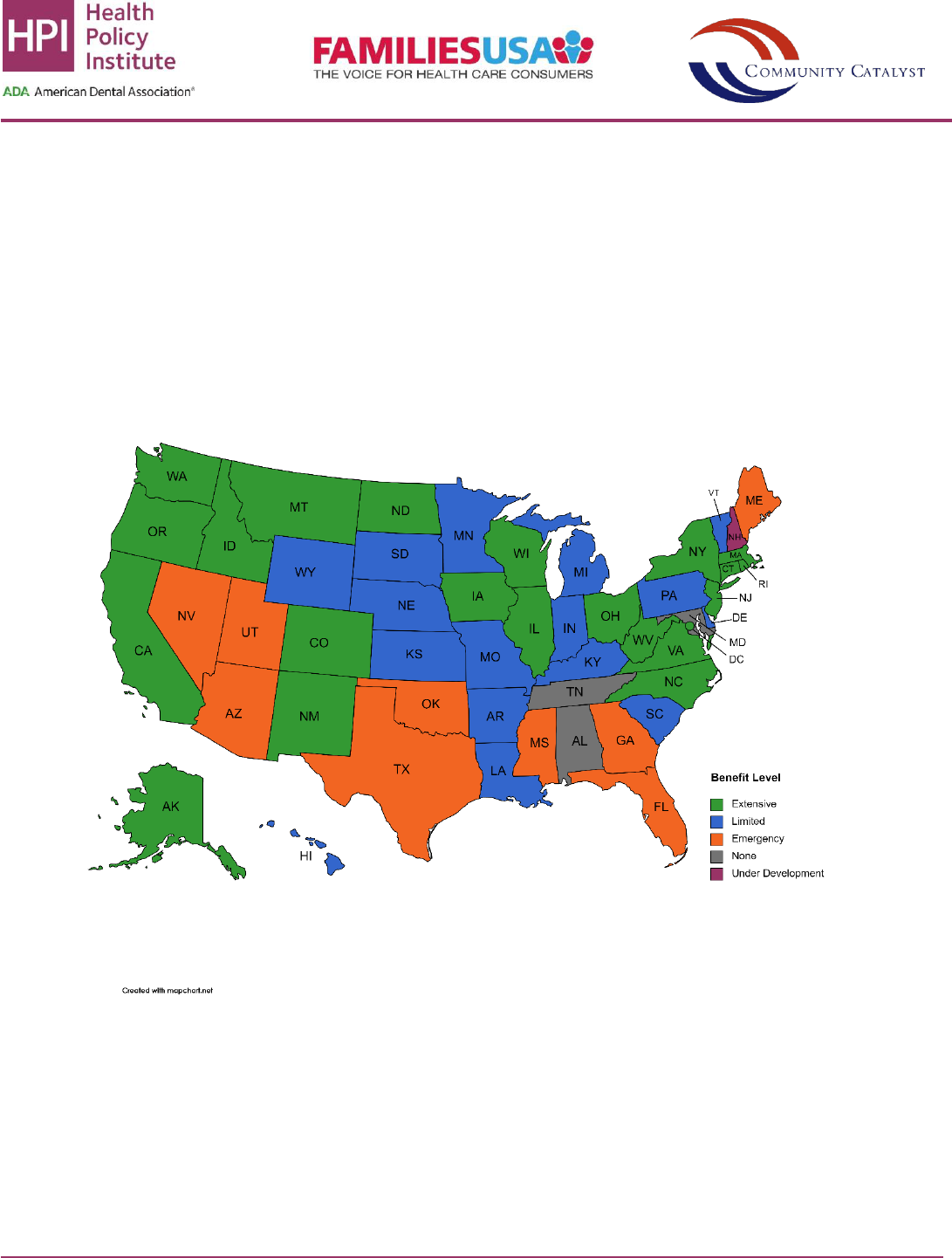
The Current Landscape of Adult
Dental Coverage within State Medicaid
Programs
Despite the overwhelming evidence of major costs
barriers to dental care among low-income adults and
the importance of coverage in alleviating cost barriers,
many states still do not provide adequate Medicaid
adult dental benefits. As of early 2021, 21 states and
the District of Columbia provide extensive adult dental
benefits in their Medicaid programs. Sixteen states
provide limited benefits, nine provide emergency-only
benefits, three provide no benefits, and one has a
dental benefit under development.
18
(Figure 2).
All states are required to comply with the Early and
Periodic Screening, Diagnostic and Treatment
(EPSDT) benefit to provide preventive and medically
necessary comprehensive health care services for
children under age 21 enrolled in Medicaid and the
Children’s Health Insurance Program (CHIP), including
dental care.
19
EPSDT offers a crucial guide to states in
5
the design of dental benefits packages for children: a
minimally acceptable set of services at its worst and a
north star of comprehensive, timely, individualized
dental care at its best – while still allowing flexibility to
align with the needs, resources, and capacities of each
individual state. There is no corresponding dental care
requirement for adult Medicaid enrollees; adult dental
coverage is optional under state Medicaid programs.
20
When a Medicaid-enrolled child enters adulthood, their
medical coverage transitions relatively seamlessly.
This does not hold true for dental care. In many states,
dental coverage is abruptly curtailed or taken away
entirely from Medicaid enrollees at the arbitrary age of
21.
Figure 2: Adult Medicaid Dental Benefit Level by State
Source: Health Policy Institute analysis of data from Center for Health Care Strategies, Inc.
18
Authors have updated the analysis with
data as of early 2021. Note: None = No coverage. Emergency-only = Coverage for pain relief under defined emergency situations.
Limited = Coverage for a subset of diagnostic, preventive, and minor restorative procedures with a per-enrollee annual maximum
expenditure of $1,000 or less. Extensive = Coverage for a more comprehensive mix of services, including at least 100 diagnostic,
preventive, and restorative procedures, and a per-enrollee annual maximum expenditure of at least $1,000.

6
Even in states that offer dental coverage for adults,
there are limits on the covered services or caps on the
amount of care enrollees can receive. Limited
coverage may focus on prevention or emergency care,
but does little to restore and/or maintain oral health for
Medicaid enrollees to prevent more severe and costly
oral disease. States’ decisions not to offer meaningful
dental coverage are usually based on fiscal
considerations that overlook potential cost savings,
and oral health benefits have historically been cut in
tight budget years. Dental benefits for adults have
neither been considered a “mandatory service” within
Medicaid nor an “essential health benefit” under the
Affordable Care Act.
21
Estimating the Cost to Provide
Extensive Adult Dental Coverage in
Medicaid in all States
We estimated the cost of providing adult dental
coverage in all state Medicaid programs. This involved
estimating the impact of adding extensive adult dental
coverage in the 28 state Medicaid programs that
currently provide either no coverage, emergency-only
coverage, or limited coverage. We estimated the
increased dental care costs as well as the offsetting
medical care cost savings from diabetes, heart
disease, and pregnancy – three conditions for which
there is reasonable evidence linking improved access
to dental care with medical cost savings. We estimated
both the federal and state government shares of
spending. Due to data constraints, we were not able to
estimate the cost savings from reductions in
emergency department use for dental conditions. Thus,
our analysis is conservative, erring on overestimating
the net cost. The detailed methodology is in Appendix
A. We summarize the key findings here.
Across all 28 state Medicaid programs, the net cost of
providing extensive dental coverage to adults is $836
million per year. This includes an estimated $1.1 billion
per year in dental care costs and $273 million per year
in medical care savings. (Table 1).
Detailed state-by-state estimates are available in
Appendix B. For example, the estimated annual state
share of new dental care spending that would be
required to introduce an extensive adult dental benefit
in Medicaid ranges from $525,511 (South Dakota) to
$51,617,933 (Pennsylvania), with an average of
$14,338,362. The state share of reduction in annual
medical care costs range from $111,816 (Wyoming) to
$17,020,266 (Texas), with an average of $3,589,406.
The net annual cost to a state of adding an extensive
benefit ranges from $255,095 (Missouri) to
$46,252,487 (Pennsylvania), with an average of
$10,748,957.
Table 1: Estimated Additional Cost of Providing Extensive Medicaid Adult Dental Benefits in All States
Dental care
spending
Medical care
savings
Net cost
State share
$401,474,150
$100,503,357
$300,970,792
Federal share
$707,533,813
$172,623,476
$534,910,337
Total
$1,109,007,963
$273,126,834
$835,881,130
Per enrollee per month
$6.16
$1.52
$4.64
Note: Table reflects net cost estimates for 28 states combined that currently have no, emergency-only, or limited adult
Medicaid dental benefits. Estimates are annual. Due to data constraints, estimates do not include expected reductions in
emergency department spending for dental conditions. See Appendix A for full methodology.

7
From Analysis to Action
Improving Medicaid adult dental coverage is a sound
investment in health, economic opportunity, and racial
equity. If all states were to provide extensive dental
benefits, we would overcome some of the enormous
barriers that low-income adults currently face. Under
the current landscape, basic access to dental care is
generally higher in states with more comprehensive
Medicaid dental benefits. Therefore, a person’s oral
health – and thus overall health and economic
opportunity – is dependent upon where they live.
The fact that Medicaid adult dental coverage remains
optional for states exacerbates deep racial and
geographic disparities in access to oral health care and
oral health outcomes. It also perpetuates inequities in
chronic disease prevalence, maternal health,
employment opportunity, and economic mobility. The
communities most affected by the COVID-19 pandemic
also face the highest barriers to accessing the oral
health care they need to be healthy and function in
their daily lives. Black, Hispanic, and other
communities of color, as well as people in rural
communities and people with disabilities, stand to
benefit most from comprehensive adult dental
coverage in Medicaid.
The optional status of Medicaid adult dental coverage
means that states can take away these benefits at any
time. Medicaid adult dental benefits are often subject to
state budget cuts during economic downturns,
especially in states with more comprehensive
coverage. It also means that states may offer different
oral health coverage to people in different eligibility
categories, such as pregnant people or people with
disabilities. This narrow definition of benefits can be
confusing for enrollees and oral health providers,
especially when covered services change with state
budget fluctuations.
Recommendations
These problems, combined with this research, provide
important considerations for federal policy change
around oral health coverage in Medicaid. The most
straightforward way to address oral health access is
through federal policy that makes comprehensive oral
health coverage for adults a permanent part of the
Medicaid program for all states.
Congress can designate dental services as a
mandatory benefit category for all Medicaid-enrolled
adults. This statutory policy change would ensure that
all states offer comprehensive oral health coverage,
eliminating the extreme variation across states. It
would also reduce or eliminate the need for states,
providers, and enrollees to differentiate between
eligibility categories for the purposes of covering dental
services. This would further reduce uncertainty for
people who may currently only have access to dental
care during pregnancy or 60 days postpartum, and
may also serve to reduce the state administrative
burden of differentiating benefits for separate
categories of Medicaid enrollees.
In order to achieve the projected increases in oral
health care access, health outcomes, and cost savings
in this model, Congress could also consider policy
aimed at establishing a baseline of
comprehensiveness for adult dental services in
Medicaid. Policymakers can amend the current
statutory definition of Medicaid dental services to
address the full range of oral health conditions,
specifying categories of services as necessary.
Previous legislation, including the Comprehensive
Dental Reform Act of 2015, the Oral Health for Moms
Act, and the Mothers and Offspring Mortality and
Morbidity Awareness Act, have taken similar
approaches in defining oral health coverage for
pregnant and adult populations in Medicaid and CHIP.
In addition to expanding the statutory definition of

8
dental services, Congress may also rely on further
specification at the regulatory level, which would likely
be carried out by the Centers for Medicare and
Medicaid Services.
Another important federal policy consideration is
bolstering state budgets as states implement oral
health coverage. While our research is based on
existing Federal Medical Assistance Percentages
(FMAP) to determine state and federal costs, Congress
could consider increasing the FMAP for states to
support comprehensive oral health coverage.
Adequate funding of state Medicaid programs is
necessary for the successful implementation of a new
benefit.
Each of these policy options would make
improvements to our current patchwork of Medicaid
adult dental coverage, and the most thorough
approach would be to implement all three together.
Regardless of what solutions federal policymakers
consider, our research shows that they should also
take into account the full range of savings that oral
health policy change can offer. History shows that state
policymakers’ fiscal calculations around oral health
coverage are often shortsighted, failing to take into
account the costs to both governments and patients of
untreated dental disease, care sought in emergency
departments, and the impact of untreated oral health
problems on other chronic conditions. As shown in our
model, improving oral health coverage not only
improves enrollees’ health, but also reduces overall
medical care costs. Notably, while limitations in the
data meant that our model could not account for
potential cost savings associated with reductions in
emergency department visits at the state level, existing
literature estimates that up to 78 percent of these visits
could be diverted to more appropriate care settings
and the cost savings could be over $1,200 per visit.
15
The savings we estimate are therefore likely
conservative.
Even without federal action, this research is instructive
for states that do not currently provide extensive dental
benefits to people who rely on Medicaid. State
policymakers can improve their states’ Medicaid adult
dental benefits, as several have in recent years, and
realize these same potential improvements in access
to care and medical care cost savings.
This analysis required making several key assumptions
that, although guided by the best available evidence
and data, are subject to uncertainty. Nevertheless, we
feel we have incorporated the best available evidence
and data to guide our modeling. The analysis is meant
to assist policymakers in assessing the need for and
the fiscal impact of ensuring a comprehensive adult
dental benefit is available in all state Medicaid
programs. The Health Policy Institute, Families USA,
and Community Catalyst are eager to work with
policymakers on initiatives that will expand access to
dental care and promote oral health equity.
About the Authors
Marko Vujicic is chief economist and senior vice
president of the Health Policy Institute of the American
Dental Association. Vujicic previously worked for the
World Health Organization and World Bank. Chelsea
Fosse is a senior health policy analyst for the Health
Policy Institute of the American Dental Association and
a licensed dentist. Colin Reusch is a senior advisor for
oral health policy for Community Catalyst’s Dental
Access Project. Reusch previously served as director
of policy for the Children’s Dental Health Project
(CDHP). Melissa Burroughs is associate director for
strategic partnerships for Families USA., leading the
Oral Health for All Campaign.

9
Appendix A
Methods for Estimating the Cost of Comprehensive Adult Dental Coverage in Medicaid Programs in All
States
Baseline Adult Dental Benefit, Dental Care Use Rate, and Estimated Total Dental Care Costs by State
We utilized previously published classifications of each state’s Medicaid adult dental benefit: none, emergency-only,
limited, or extensive.
18
Emergency-only states cover pain relief under defined emergency situations. Limited states
cover a subset of diagnostic, preventive, and minor restorative procedures with a per-enrollee annual maximum
expenditure of $1,000 or less. Extensive states cover a more comprehensive mix of services, including at least 100
diagnostic, preventive, and restorative procedures, and a per-enrollee annual maximum expenditure of at least
$1,000.
18
Classifications from 2018 were used for baseline.
22
For the current benefit classifications, we updated the classification
for states that underwent changes to their benefits packages since the most recent publication (2019), including Alaska,
Virginia, and West Virginia, which have or will have extensive benefits in place in 2021. This also included Delaware,
which now has a limited benefit. In this research brief, we focus our modeling on the 28 states with no, emergency-only,
or limited Medicaid adult dental benefits. Utah is excluded from our analysis for data reasons mentioned below.
We relied on Medicaid de-identified claims data from the Transformed Medicaid Statistical Information System (T-
MSIS), maintained by the U.S. Centers for Medicare and Medicaid Services (CMS), to assess utilization of and
expenditures for dental services among Medicaid-enrolled adults.
23
Since 2014, states have provided T-MSIS detailed
information regarding Medicaid and CHIP enrollment, service utilization, and payments. As of 2018, all states and the
District of Columbia provide T-MSIS with claims data on a monthly basis. The most recent year of T-MSIS data
available is from 2018. Thus, 2018 was selected to calculate baseline utilization and expenditures. Dental claims are
contained in the other services (OT) claims tables, one of the T-MSIS Analytic Files (TAFs) housed in the Chronic
Condition Warehouse (CCW).
24
This research is part of a data use agreement (DUA) approved by CMS (DUA RSCH-
2020-5563: “The State of Oral Healthcare Use, Quality and Spending: Findings from Medicaid and CHIP Programs”).
We extracted all dental procedure codes that appear in the American Dental Association’s Codes on Dental Procedures
and Nomenclature (CDT) manual from the 2018 T-MSIS OT Medicaid tables.
25
For each state, we measured dental
care utilization as the proportion of enrolled individuals who had at least one dental claim in the year. Specifically, to
produce a state-level utilization rate, we compared the number of enrollees age 21 and over who were enrolled for 365
days and had any dental claim in the year to the total number of adult Medicaid enrollees who were enrolled for 365
days. Dental visits that took place in an emergency department were not included. We used the claim type indicator
variable from the OT header table to differentiate between managed care and fee-for-service (FFS) claims; payment
data is available for FFS claims, but not managed care claims. We aggregated the FFS payments for dental services
for all enrollees age 21 and over by state and calculated the average annual expenditure per dental patient (adult with
any dental claim in the year).

10
There is no baseline expenditure data available for Utah because all dental services are paid for under managed care
and not reported in T-MSIS, which inhibits its inclusion in the modeling. Therefore, Utah is excluded from our analysis.
We obtained Medicaid enrollment figures from CMS.
26
These data provide monthly enrollment by state, including total
Medicaid and CHIP enrollment and total Medicaid and CHIP child enrollment. We used data from December 2018 for
baseline and August 2020 (the most recently available final enrollment figures) for post-reform enrollment projections.
For most states, we estimated Medicaid adult enrollment by subtracting the child enrollment from the total enrollment.
Child enrollment data were missing for Tennessee in 2018 and for Arizona in 2018 and 2020. To address this data
shortcoming, we used CMS-416 data for 2018 and 2019, the most recent available, as the source for child enrollment
estimates for Arizona and Tennessee. We then subtracted that estimate from total enrollment to reach adult
enrollment.
27
Baseline Dental Care Use and Per Patient Spending by Classification of Adult Dental Benefit
To estimate the additional cost to the Medicaid program of introducing “extensive” adult dental benefits, we estimated
how many Medicaid adult enrollees would use dental care services in a given year after an adult dental benefit is
introduced and how much, on average, would be spent on each dental care patient. An “extensive” Medicaid adult
dental benefit is defined as a benefit that covers 100 or more dental procedures and has an annual benefit maximum at
or above $1,000 per patient per year.
18
We recognize there are significant drawbacks to this simplistic definition, but
there is not an alternative definition that has been published in the literature.
Evidence indicates that when adults covered by Medicaid have dental coverage newly available to them, there is an
increase in dental care use.
8,
28
,
29
,
30
This may occur through the enhancement of an existing adult dental benefit (such
as from limited to extensive) or when additional adults become eligible for Medicaid (such as through income eligibility
with Medicaid expansion). Research has shown that the rate of dental care use increases in the range of 6-10
percentage points within one year of implementation of extensive benefits.
8,28,29
Adults with more generous benefits
packages are more likely to use dental care.
31
In our analysis, we assumed that the change in utilization in any given state will be dependent on the degree of benefit
change with the implementation of an extensive benefit. In other words, we predict there will be a greater increase in
utilization in states that currently have no adult dental benefit and implement an extensive benefit, compared to states
that currently have a limited benefit that is enhanced to be comprehensive. In Appendix A Table 1, we calculated the
average dental care utilization rate among Medicaid-enrolled adults by adult dental benefit type. The mean utilization at
baseline for all states with no adult dental benefit 0.9% percent, the mean utilization at baseline for all states with an
emergency-only adult dental benefit is 9.2 percent, and the mean utilization at baseline for all states with a limited adult
dental benefit is 21.8 percent. We compared the average utilization for each of the no benefit, emergency-only benefit,
and limited benefit groups to the average utilization in states with an extensive benefit.

11
Appendix A, Table 1: Utilization, Expenditures by Type of Adult Medicaid Dental Benefit
Adult Dental Benefit
Classification at
Baseline
Number of
States
Average Baseline
Utilization
Utilization
Difference
Compared to
Extensive
Average Annual
Expenditures Per
Patient
None
3
0.9%
27.5%
$784
Emergency
13
9.2%
19.2%
$445
Limited
16
21.8%
6.5%
$281
Extensive
19
28.4%
--
$437
Source: Health Policy Institute analysis of data obtained from the Transformed Medicaid Statistical Information System
(T-MSIS), maintained by the U.S. Centers for Medicare and Medicaid Services (CMS).
The average percentage of Medicaid adults with a dental visit in a year across extensive states in 2018 was 28.4
percent. We used these differences (none vs. extensive, emergency-only vs. extensive, limited vs. extensive) to
calculate the state-specific increase in utilization with the implementation of an extensive benefit based on its baseline
utilization. We added 27.5 percent to the baseline dental care utilization rate for states without an adult dental benefit
(including New Hampshire, where the dental benefit is under development), 19.2 percent for states with an emergency-
only benefit, and 6.5 percent for states with an existing limited adult dental benefit.
We used a single estimate for dental expenditures per dental patient following the implementation of an extensive adult
dental benefit based on analysis of T-MSIS data. We used the average total dental expenditure paid by Medicaid
among Medicaid-enrolled adults with a dental visit within the year, averaged across states that provided an extensive
adult dental benefit in Medicaid in 2018. This yielded an average expenditure level of $437 per dental care patient per
year. We assumed that all expenditures related to implementing an extensive adult dental benefit are paid for by the
Medicaid program; we did not account for the possibility of patient copays or coinsurance.
In summary, to calculate the total incremental expenditure of implementing an extensive Medicaid adult dental benefit,
we used the following formula for each state:
Expenditure = Enrollment * Utilization Rate * Spending Per User
Post-Reform Projected Dental Care Use and Dental Care Spending
To determine the federal and state shares of the estimated Medicaid expenditures, we used the most recent (fiscal year
2021) federal medical assistance percentage (FMAP) for Medicaid.
32
In states that have expanded Medicaid eligibility, a greater share of the cost of services for the expansion population is
paid by the federal government. We did not factor this into the state and federal shares and recognize this as a potential
shortcoming. However, given this adjustment, Medicaid expansion states would see a lower share of expenditures
attributed to their state budgets.
Post-Reform Estimated Reduction in Medical Care Costs
We estimated medical care cost reductions associated with increased access to dental care for adult Medicaid
enrollees. There is emerging evidence that increased access to dental care can lead to lower health care costs among
pregnant patients and patients with chronic conditions such as diabetes and heart disease.
16,17

12
Medical Care Cost Savings: Emergency Department Visits
The national average cost of an emergency department (ED) visit for a dental condition is $1,286.
33
The available
evidence suggests that up to 78 percent of ED visits for dental conditions nationwide could be diverted to a dentist
office or other ambulatory setting.
34
A recent study demonstrated a 14 percent reduction in dental-related ED visits one
year after expanding dental benefits via Medicaid expansion.
28
For methodological reasons, we did not include in this analysis the savings from reductions in ED use for dental
conditions. The costs for dental-related ED visits are not included in the baseline dental spending due to the
construction of these expenses in the T-MSIS dataset. Therefore, we did not model the offsets. Thus, our baseline
spending is an underestimate in terms of total dental care spending without the inclusion of ED associated costs of
dental care. However, additional savings would be projected due to the diversion of ED-based dental care to more cost-
effective and clinically appropriate settings when adult enrollees have an extensive adult dental benefit.
14,15,34
Medical Care Cost Savings: Diabetes and Coronary Artery Disease
We estimated the number of Medicaid enrollees in each state who have diabetes and coronary artery disease based on
the share nationally of adult Medicaid enrollees who have these health conditions. In the most recent year reported
(2018), 11.4 percent of Medicaid enrollees nationwide self-reported they had diabetes and 3 percent reported they had
coronary artery disease.
35
We applied the national rates for these chronic conditions among Medicaid enrollees to all
states. We assumed adults with these conditions will behave similarly in terms of their dental care seeking behavior
when an extensive dental benefit for adults is introduced. In other words, their dental care utilization rate will increase
by the same amount as adult enrollees in general.
We assumed that 60 percent of adult Medicaid enrollees have some form of periodontal disease. This estimate is
based on the most recent national data on the prevalence of periodontal disease among low-income adults in the U.S.
36
This 60 percent estimate also applies to pregnant enrollees.
37
Based on the available evidence, estimated medical costs would be reduced between $900
17
and $2,840
16
per patient
with diabetes who receives periodontal treatment. We used the lower end of this range and assumed a medical care
cost reduction of $900 per year for each new dental patient with diabetes once in a “steady state.” The available
evidence suggests that medical cost savings among adults with coronary artery disease who receive periodontal
treatment are $1,090
16
per year.
Medical Care Cost Savings: Pregnancy
We utilized the most recently available (2018) state-level data on the number of births among Medicaid,
38
but
subtracted the number of teen births by state.
39
Approximately 77.5 percent of teen births nationally are paid for by
Medicaid,
38
so that share of 2018 teen births were subtracted from each states’ total overall births to produce an
approximate number of pregnancies in Medicaid in each state. We assumed that pregnant enrollees will behave
similarly in terms of their dental care seeking behavior when a dental benefit for adults is introduced into Medicaid,
meaning their utilization rate will increase by the same amount as other adult enrollees.

13
Based on the available evidence, the estimated medical cost savings are between $1,500 (second pregnancy) and
$2,400 (first pregnancy) per year per pregnant woman receiving periodontal treatment.
16
For our modeling, we chose
the low end of this range and assumed a medical cost reduction of $1,500 per year per pregnant enrollee.
In summary, the medical care spending offsets for these various conditions is estimated using the following formula:
Medical Care Offset = Enrollees * Change in Utilization Rate * Share of Enrollees with Condition * Share with Condition
with Periodontal Disease * Medical Care Costs
Similar to the new dental care costs, we used the FMAP to distribute these medical care cost offsets across state and
federal budgets.
Cost of Adding an Extensive Dental Benefit by State
The impact of introducing comprehensive adult dental benefits in Medicaid, particularly the medical cost savings, is not
immediate. There is very little research to draw on to predict when these costs and savings would be realized following
the implementation of comprehensive benefits and how long this takes in practice. Enrollees become aware of the
benefit gradually, providers need time to adjust,
40
and medical care cost reductions are not realized immediately. For
simplification purposes, our analysis does not account for these time lags. Rather, it is best interpreted as “steady state”
estimate, likely to be most accurate over a two to five-year timeframe.

14
Appendix B
Estimated Cost of Comprehensive Adult Dental Coverage in Medicaid Programs in All States without an
Extensive Benefit
Baseline
dental
benefit for
adults
Adult
Medicaid
enrollment
Baseline
dental
care
utilization
rate
Projected
dental
care
utilization
rate
Additional
dental care
spending
Additional
medical
care
savings
Net cost
Net
Cost
per
enrollee
per
month
State
share
of net
cost
Alabama
None
283,788
0.1%
27.6%
$34,124,292
$12,782,664
$21,341,628
$6.27
27.6%
Maryland
None
759,189
13.3%
40.8%
$57,275,116
$23,521,013
$33,754,102
$3.71
50.0%
Tennessee
None
667,145
1.3%
28.8%
$77,896,427
$23,536,106
$54,360,321
$6.79
33.6%
New
Hampshire
Under
Development
105,181
7.5%
35.0%
$13,778,918
$3,048,687
$10,730,231
$8.50
50.0%
Arizona
Emergency
933,564
4.4%
23.6%
$93,699,447
$21,444,043
$72,255,404
$6.45
30.0%
Florida
Emergency
1,372,790
8.8%
28.0%
$97,020,830
$38,916,328
$58,104,502
$3.53
39.0%
Georgia
Emergency
604,272
9.6%
28.8%
$53,774,304
$18,686,512
$35,087,793
$4.84
33.2%
Maine
Emergency
127,662
10.7%
29.9%
$12,226,687
$2,763,428
$9,463,259
$6.18
36.0%
Mississippi
Emergency
211,101
11.4%
30.6%
$20,182,841
$6,940,708
$13,242,133
$5.23
21.7%
Nevada
Emergency
389,234
18.9%
38.1%
$21,691,113
$8,732,803
$12,958,309
$2.77
37.4%
Oklahoma
Emergency
259,116
9.2%
28.4%
$25,661,338
$8,052,508
$17,608,830
$5.66
31.7%
Texas
Emergency
997,541
5.3%
24.5%
$78,362,115
$43,419,045
$34,943,070
$2.92
39.2%
Arkansas
Limited
467,719
9.8%
16.3%
$24,152,533
$3,323,919
$20,828,614
$3.71
28.4%
Delaware
Limited
134,263
1.1%
7.6%
$3,142,452
$969,724
$2,172,729
$1.35
42.3%
Hawaii
Limited
214,504
8.1%
14.6%
$9,236,674
$1,423,569
$7,813,105
$3.04
46.4%
Indiana
Limited
813,254
26.6%
33.1%
$42,446,948
$6,040,819
$36,406,130
$3.73
33.7%
Kansas
Limited
124,954
17.0%
23.5%
$7,655,024
$1,241,970
$6,413,054
$4.28
39.8%
Kentucky
Limited
908,740
18.5%
25.0%
$68,802,428
$6,151,205
$62,651,223
$5.75
27.3%
Louisiana
Limited
886,412
14.1%
20.6%
$76,783,758
$6,736,875
$70,046,882
$6.59
32.0%
Michigan
Limited
1,529,074
26.1%
32.6%
$119,011,070
$10,586,689
$108,424,381
$5.91
34.5%
Minnesota
Limited
563,718
36.6%
43.1%
$18,673,023
$4,171,782
$14,501,241
$2.14
49.5%
Missouri
Limited
365,003
16.7%
23.2%
$4,129,885
$3,371,576
$758,309
$0.17
33.6%
Nebraska
Limited
91,781
37.0%
43.5%
$9,359,136
$951,469
$8,407,667
$7.63
42.2%
Pennsylvania
Limited
1,692,591
26.2%
32.7%
$109,082,699
$11,338,645
$97,744,055
$4.81
47.3%
South
Carolina
Limited
417,513
14.1%
20.6%
$21,430,923
$3,696,485
$17,734,438
$3.54
29.3%
South
Dakota
Limited
34,359
29.8%
36.3%
$1,272,115
$381,959
$890,156
$2.16
41.3%
Vermont
Limited
102,203
29.8%
36.3%
$6,673,414
$672,672
$6,000,743
$4.89
43.5%
Wyoming
Limited
21,160
20.2%
26.7%
$1,462,452
$223,631
$1,238,821
$4.88
50.0%
15
References
1
Vujicic M, Buchmueller T, Klein R. Dental care presents the highest level of financial barriers, compared to other types
of health care services. Health Aff (Millwood). 2016;1;35(12): 2176-2182.
2
Gupta N, Vujicic M. Main barriers to getting needed dental care all relate to affordability. American Dental Association.
Health Policy Institute Research Brief. April 2019. Available from: https://www.ada.org/-/media/project/ada-
organization/ada/ada-org/files/resources/research/hpi/hpibrief_0419_1.pdf. Accessed June 7, 2021.
3
American Dental Association. Dental care utilization in the U.S. Health Policy Institute Infographic. November 2017.
Available from: https://www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/HPIgraphic_1117_2.pdf.
Accessed June 7, 2021.
4
American Dental Association. Oral health and well-being in the United States. Health Policy Institute Infographic.
2015. Available from: https://www.ada.org/-/media/project/ada-organization/ada/ada-
org/files/resources/research/hpi/us-oral-health-well-being.pdf. Accessed June 7, 2021.
5
American Dental Association. Cost barriers to dental care among the U.S. population, by race and ethnicity. Health
Policy Institute Infographic. April 2021. Available from: https://www.ada.org/-/media/project/ada-organization/ada/ada-
org/files/resources/research/hpi/hpigraphic_0421_3.pdf. Accessed June 7, 2021.
6
American Dental Association. Dental care utilization among the U.S. population, by race and ethnicity. Health Policy
Institute Infographic. April 2021. Available from: https://www.ada.org/-/media/project/ada-organization/ada/ada-
org/files/resources/research/hpi/hpigraphic_0421_4.pdf. Accessed June 7, 2021.
7
Kieffer EC, Goold SD, Buchmueller T, et al. Beneficiaries' perspectives on improved oral health and its mediators after
Medicaid expansion in Michigan: a mixed methods study. J Public Health Dent. 2021. doi: 10.1111/jphd.12447.
8
Choi MK. The impact of Medicaid insurance coverage on dental service use. J Health Econ. 2011;30(5): 1020-31.
9
Edelstein BL, Rubin MS, Clouston SAP, Reusch C. Children’s dental service use reflects their parents’ dental service
experience and insurance. JADA. 2020;151(12): 935-943.
10
American Dental Association. Oral health and well-being among Medicaid adults by type of Medicaid dental benefit.
Health Policy Institute Infographic. May 2018. Available from: https://www.ada.org/-/media/project/ada-
organization/ada/ada-org/files/resources/research/hpi/hpigraphic_0518_1.pdf. Accessed June 7, 2021.
11
House DR, Fry CL, Brown LJ. The economic impact of dentistry. JADA. 2004;135(3): 347-352.
12
Graham M. Does the new tax law benefit you? Probably? JADA. 2018;149(5): 331-333.
13
Bivens J. Updated employment multipliers for the U.S. economy. Economic Policy Institute. January 23, 2019.
Available from: https://www.epi.org/publication/updated-employment-multipliers-for-the-u-s-economy/. Accessed June
7, 2021.
14
Singhal A, Caplan DJ, Jones MP, et al. Eliminating Medicaid adult dental coverage in California led to increased
dental emergency visits and associated costs. Health Aff (Millwood). 2015;34(5): 749-756.
15
Nasseh K, Vujicic M, Romaine D. Diverting emergency department dental visits could save Maryland’s Medicaid
program $4 Million per year. American Dental Association. Health Policy Institute Research Brief. November 2014.
Available from: http://www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/HPIBrief_1114_2.pdf.
Accessed June 7, 2021.
16
Jeffcoat MK, Jeffcoat RL, Gladowski PA, Bramson JB, Blum JJ. Impact of periodontal therapy on general health:
evidence from insurance data for five systemic conditions. Am J Prev Med. 2014;47(2): 166-174.
17
Nasseh K, Vujicic M, Glick M. The relationship between periodontal interventions and healthcare costs and utilization.
Health Econ. 2017;26(4): 519-527.
18
Center for Health Care Strategies, Inc. Medicaid adult dental benefits: an overview. September 2019.
https://www.chcs.org/media/Adult-Oral-Health-Fact-Sheet_091519.pdf. Accessed June 7, 2021. Updated with authors’
analysis.
16
19
Medicaid.Gov. Early and periodic screening, diagnostic, and treatment. Centers for Medicare & Medicaid Services.
Available from: https://www.medicaid.gov/medicaid/benefits/early-and-periodic-screening-diagnostic-and-
treatment/index.html. Accessed June 7, 2021.
20
Medicaid.Gov. Mandatory & optional Medicaid benefits. Centers for Medicare & Medicaid Services. Available from:
https://www.medicaid.gov/medicaid/benefits/mandatory-optional-medicaid-benefits/index.html. Accessed June 7, 2021.
21
HealthCare.Gov. What Marketplace health insurance plans cover: 10 essential health benefits. Available from:
https://www.healthcare.gov/coverage/what-marketplace-plans-cover/. Accessed June 7, 2021.
22
Center for Health Care Strategies, Inc. Medicaid adult dental benefits: an overview. July 2018. Available from:
https://www.chcs.org/media/Adult-Oral-Health-Fact-Sheet_072718.pdf. Accessed June 7, 2021.
23
Medicaid.gov. Transformed Medicaid Statistical Information System (T-MSIS). Centers for Medicare and Medicaid
Services. January 2021. Available from: https://www.medicaid.gov/medicaid/data-systems/macbis/transformed-
medicaid-statistical-information-system-t-msis/index.html. Accessed June 7, 2021.
24
Centers for Medicare and Medicaid Services. Chronic conditions data warehouse. Available at:
https://www2.ccwdata.org/web/guest/home. Accessed June 7, 2021.
25
American Dental Association. CDT 2020. Dental Procedure Codes. 2020. Available from:
https://www.ada.org/en/publications/cdt. Accessed June 7, 2021.
26
Medicaid.gov. State Medicaid and CHIP applications, eligibility determinations, and enrollment data. Centers for
Medicare and Medicaid Services. Available from: https://data.medicaid.gov/Enrollment/State-Medicaid-and-CHIP-
Applications-Eligibility-D/n5ce-jxme. Accessed June 7, 2021.
27
Medicaid.gov. Early and periodic screening, diagnostic, and treatment. Annual Reporting CMS-416 data files.
Available from: https://www.medicaid.gov/medicaid/benefits/early-and-periodic-screening-diagnostic-and-
treatment/index.html. Accessed June 7, 2021.
28
Elani HW, Sommers BD, Kawachi I. Changes in coverage and access to dental care five years after ACA Medicaid
expansion. Health Aff (Millwood). 2020;39(11): 1900-1908.
29
Lyu W, Shane DM, Wehby GL. Effects of the recent Medicaid expansions on dental preventive services and
treatments. Med Care. 2020;58(8): 749-755.
30
Wehby GL, Lyu W, Shane DM. The impact of the ACA Medicaid expansions on dental visits by dental coverage
generosity and dentist supply. Med Care. 2019;57(10): 781-787.
31
Singhal A, Damiano P, Sabik L. Medicaid adult dental benefits increase use of dental care, but impact of expansion
on dental services use was mixed. Health Aff (Millwood). 2017;36(4): 723-732.
32
Federal Register. Federal matching shares for Medicaid. Vol. 85, No. 230. U.S. Department of Health and Human
Services. Available from: https://www.govinfo.gov/content/pkg/FR-2020-11-30/pdf/2020-26387.pdf. Accessed June 7,
2021.
33
American Dental Association. Emergency department visits for dental conditions – a snapshot. Health Policy Institute
Infographic. April 2020. Available from: https://www.ada.org/-/media/project/ada-organization/ada/ada-
org/files/resources/research/hpi/hpigraphic_0420_1.pdf. Accessed June 7, 2021.
34
Wall T, Nasseh K, Vujicic M. Majority of dental-related emergency department visits lack urgency and can be diverted
to dental offices. American Dental Association. Health Policy Institute Research Brief. August 2014. Available from:
https://www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/HPIBrief_0814_1.pdf. Accessed June 7,
2021.
35
Medicaid and CHIP Payment and Access Commission. MACStats: Medicaid and CHIP Data Book. December 2019.
Available from: https://www.macpac.gov/publication/macstats-medicaid-and-chip-data-book-2/. Accessed June 7, 2021.
36
Eke PI, Thornton-Evans GO, Wei L, Borgnakke WS, Dye BA, Genco RJ. Periodontitis in US adults. JADA.
2018;149(7): 576-588.e6.
37
Centers for Disease Control and Prevention. Pregnancy and oral health. February 19, 2019. Available from:
https://www.cdc.gov/oralhealth/publications/features/pregnancy-and-oral-health.html. Accessed June 7, 2021.
38
Medicaid and CHIP Payment and Access Commission. Medicaid’s role in financing maternity care. January 2020.
Available from: https://www.macpac.gov/wp-content/uploads/2020/01/Medicaid%E2%80%99s-Role-in-Financing-
Maternity-Care.pdf. Accessed June 7, 2021.
17
39
Kids Count Data Center. Teen births by age group in the United States. Annie E. Casey Foundation. Available from:
https://datacenter.kidscount.org/data/tables/8125-teen-births-by-age-group. Accessed June 7, 2021.
40
Buchmueller T, Miller S, Vujicic M. How do providers respond to changes in public health insurance coverage?
Evidence from adult Medicaid dental benefits. Am Econ J Econ Policy. 2016;8(4): 70-102.
Suggested Citation
Vujicic M, Fosse C, Reusch C, Burroughs M. Making the case for adults in all state Medicaid programs. Health Policy
Institute White Paper. American Dental Association in partnership with Community Catalyst and Families USA. July
2021. Available from: https://www.ada.org/-/media/project/ada-organization/ada/ada-
org/files/resources/research/hpi/whitepaper_0721.pdf.
