�MARYLAND
� Department
of Health
8
MARYLAND’S 2018 ANNUAL ORAL HEALTH LEGISLATIVE REPORT
Health-General Article §13-2504(b)
Larry Hogan Boyd K. Rutherford Robert R. Neall
Governor Lt. Governor Secretary
Table of Contents
Executive Summary 3
I. Introduction 4
II. Maryland’s Oral Health Accomplishments 5
Part 1. Oral Health Safety Net Program 5
Community Programs Supported 5
Federally-Funded Grant Projects 7
Expanding Oral Health Infrastructure 8
Part 2. Medicaid Dental Care Access 11
Availability and Accessibility of Dentists in Medicaid 12
Maryland Healthy Smiles Dental Program Dental Utilization Rates 14
HealthChoice Dental Utilization Rates 16
Emergency Department Utilization 18
Recent Dental Legislation and Program Expansions 19
III. Conclusion and Future Initiatives 20
Appendix A: Glossary of Key Abbreviations 21
Appendix B: Medicaid Dental Funding, Expenditures, and Utilization Rates; MCO and
Maryland Healthy Smiles Dental Program Funding and Expenditures for Dental Services; and
Utilization of Dental Services in HealthChoice and DentaQuest, SFY 1997 - CY 2017 22
Appendix C: State Public Health Dental Programs 23
Appendix D: Map of Maryland Health Professional Shortage Areas as of August 2018 26
Appendix E: Medicaid Dental Utilization Rates, CY 2004 – CY 2017 (Enrollment in Medicaid >
320 Days*, Ages 4-20) 27

2018 Annual Oral Health Legislative Report
Page 3
Executive Summary
The Centers for Medicare and Medicaid Services (CMS) and other stakeholders recognize
Maryland as a national leader in oral health.
1
Maryland has implemented programs to improve
access to oral health services through changes to the Maryland Medical Assistance Program
(Medicaid) and by expanding public health dental infrastructure. Maryland continues to receive
high grades from the federal government for its oral health initiatives because of its resolute
efforts to improve dental care access for low-income Marylanders, especially those who are
Medicaid-eligible, underserved, or underinsured.
The Maryland Department of Health (the Department) intends to focus its oral health
improvement efforts to address gaps in oral health literacy, improve disease prevention, and
increase availability and access to quality dental care in Maryland. The Department’s Office of
Oral Health (OOH) also continues to address other key issues, including provider access and
ensuring children across the state have access to preventive services, such as dental sealants and
fluoride varnish. Medicaid continues to see increases in the number of providers and in
utilization of dental care. Also, Medicaid is in the process of implementing a new adult dental
pilot that will provide services to adults ages 21 through 64 who are eligible for both Medicaid
and Medicare.
Oral Health Safety Net Program
The Governor included $1.3 million in the state fiscal year (SFY) 2018 budget for OOH to
continue to support community-based oral health grants. These grants aim to expand the dental
public health capacity for low-income, disabled, and Medicaid-eligible populations. Building on
prior successes, this additional funding provides Marylanders in every jurisdiction access to a
public health dental clinic that serves their area.
The Department is also required to provide education on oral cancer prevention for high-risk,
underserved populations. The Oral Cancer Initiative, mandated by Chapters 307 and 308 of the
Acts of 2000 (House Bill (HB) 1184/SB 791), requires that the Department implement programs
to train health care providers on oral cancer screening and referral of patients with oral cancer to
appropriate service providers.
Medicaid Dental Care Access
Maryland’s Medicaid dental benefits, collectively called the Maryland Healthy Smiles Dental
Program, are administered by a single statewide dental administrative services organization
(ASO). The ASO is responsible for coordinating all dental services for children, pregnant
women, adults in the Rare and Expensive Case Management (REM) Program, and former foster
care youth up to the age 26. Additionally, the ASO is responsible for all functions related to the
delivery of dental services for these populations, including provider network development and
1
Centers for Medicare and Medicaid Services, “CMCS Informational Bulletin: Update on CMS Oral Health
Initiative and Other Oral Health Related Items,” 10 July 2014, Department of Health and Human Services, 10
October 2017. https://www.medicaid.gov/Federal-Policy-Guidance/Downloads/CIB-07-10-2014.pdf

2018 Annual Oral Health Legislative Report
Page 4
maintenance, claims processing, utilization review, authorization of services, outreach and
education, and complaint resolution. Scion Dental, LLC (Scion) has been serving as the ASO
since calendar year (CY) 2016 after a re-procurement of the contract in 2015.
Medicaid spent $186.8 million for dental expenditures in CY 2017 (see Appendix B). Utilization
rates have increased and provider networks have expanded since the Department improved and
rebranded its dental benefit as the Maryland Healthy Smiles Dental Program. Maryland dental
utilization continues to outpace national averages.
The Department is also pursuing opportunities to continue to expand service coverage to
vulnerable adults. On May 15, 2018, Governor Hogan signed Senate Bill (SB) 284 - Maryland
Medical Assistance Program - Dental Coverage for Adults - Pilot Program (Chapter 621 of the
Acts of 2018) into law. The law requires the Department to implement an adult dental pilot
program. The Department is proposing a limited adult dental pilot that will serve individuals
statewide who are eligible for both Medicare and Medicaid (dual eligibles) and are 21 through 64
years of age. The proposed statewide pilot program will serve approximately 38,510 individuals
who currently do not receive dental services. The proposed dental package includes coverage for
diagnostic, preventive, and restorative services, in addition to extractions. The target start date is
the first half of 2019. Program regulations are currently in development at the Department. As
mandated in SB284, the objective in implementing this pilot is to determine whether offering an
adult dental benefit will improve health outcomes for vulnerable adults.
I. Introduction
Pursuant to Health-General Article §13-2504(b), Annotated Code of Maryland, the Maryland
Medical Assistance Program (Medicaid) and the Office of Oral Health (OOH) within the
Maryland Department of Health (the Department) are required to submit a comprehensive oral
health report that addresses the following areas:
1) The results of the Oral Health Safety Net Program administered by OOH;
2) Findings and recommendations for the Oral Health Safety Net Program and OOH’s Oral
Cancer Initiative;
3) The availability and accessibility of dentists throughout the state participating in
Medicaid;
4) The outcomes that managed care organizations (MCOs) and dental MCOs under
Medicaid achieve concerning the utilization of targets required by the Five Year Oral
Health Care Plan,
2
including:
(a) Loss ratios that the MCOs and dental MCOs experience for providing dental
services; and
2
The Five Year Oral Health Plan was established by Chapter 113 of the Acts of 1998 (Senate Bill 590) and at the
time established five consecutive years of dental access targets starting in 1998 when dental access was expected to
increase by 10 percent each year. This iteration of the Plan concluded in 2003 and information related to the targets
set by the 1998 Plan will not be included in this report. Currently, the dental ASO is the primary provider of dental
services; MCOs may provide a limited dental package to their members. There is no dental MCO.

2018 Annual Oral Health Legislative Report
Page 5
(b) Corrective actions taken by MCOs and dental MCOs to achieve the utilization
targets; and
5) The allocation and use of funds authorized for dental services under Medicaid.
II. Maryland’s Oral Health Accomplishments
Part 1. Oral Health Safety Net Program
Improving access to oral health services requires multiple strategies. Chapters 527 and 528 of the
Acts of 2007 (HB 30/SB 181) established the Oral Health Safety Net Program within the Office
of Oral Health (OOH). The purpose of the program is to:
1) Support collaborative and innovative ways to expand oral health capacity for low-
income, disabled, and Medicaid populations by awarding community-based oral health
grants to local health departments (LHDs), federally-qualified health centers (FQHCs),
and other non-profit entities providing oral health services within State facilities;
2) Contract with a licensed dentist to provide public health expertise for the State; and
3) Provide continuing education courses on oral health to healthcare providers.
OOH continues to explore new and creative strategies to enhance the oral health safety net,
including:
1) Providing new or expanded oral health services in publicly-funded federal, state, or local
programs;
2) Developing public and private partnerships; and
3) Expanding school-based and school-linked dental programs.
Community Programs Supported
OOH supports several community programs in LHDs, FQHCs, hospitals, and foundations across
the State targeting underserved areas and individuals with unmet need. By leveraging funding
from OOH as well as additional sources, these community programs are able to positively impact
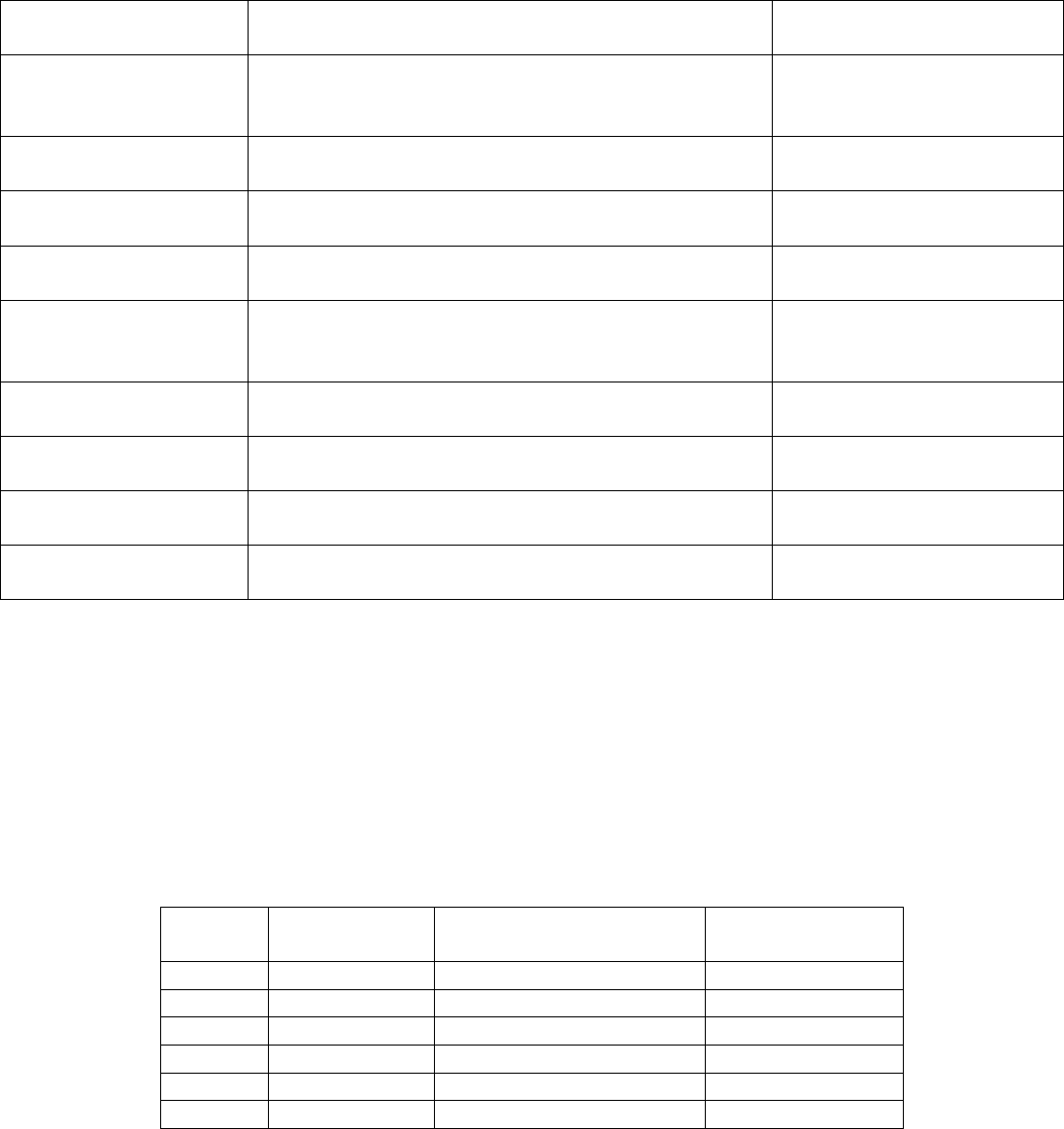
every county in Maryland through a diverse set of initiatives (see Table 1).
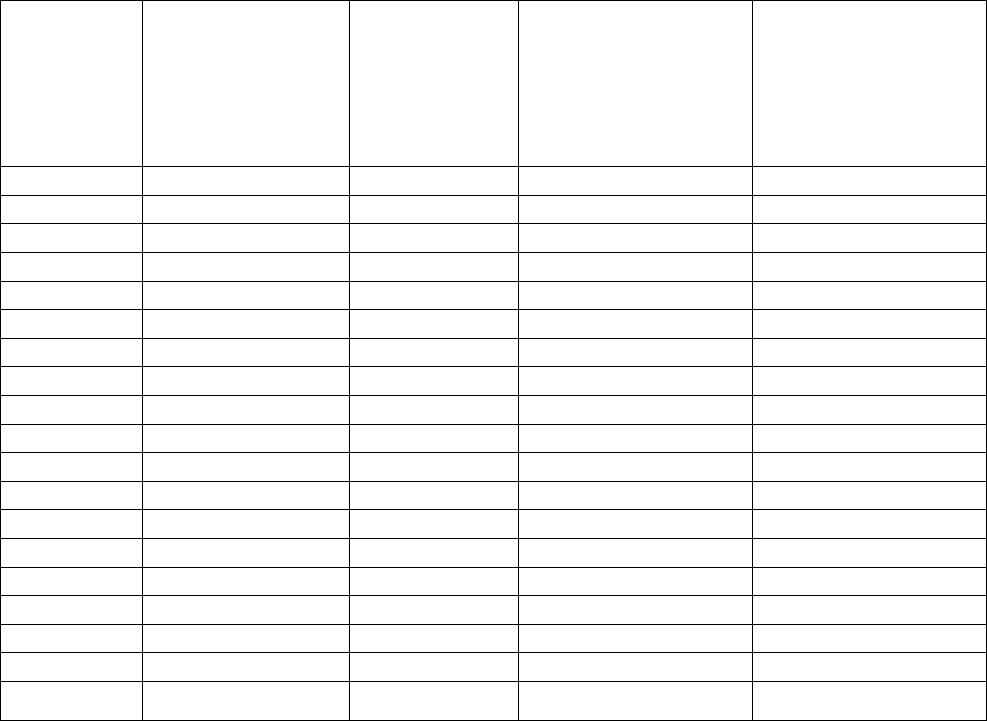
Table 1: Community Programs Supported, SFY 2018
Program
County(ies)
Activities
Impact
2018 Annual Oral Health Legislative Report
Page 6
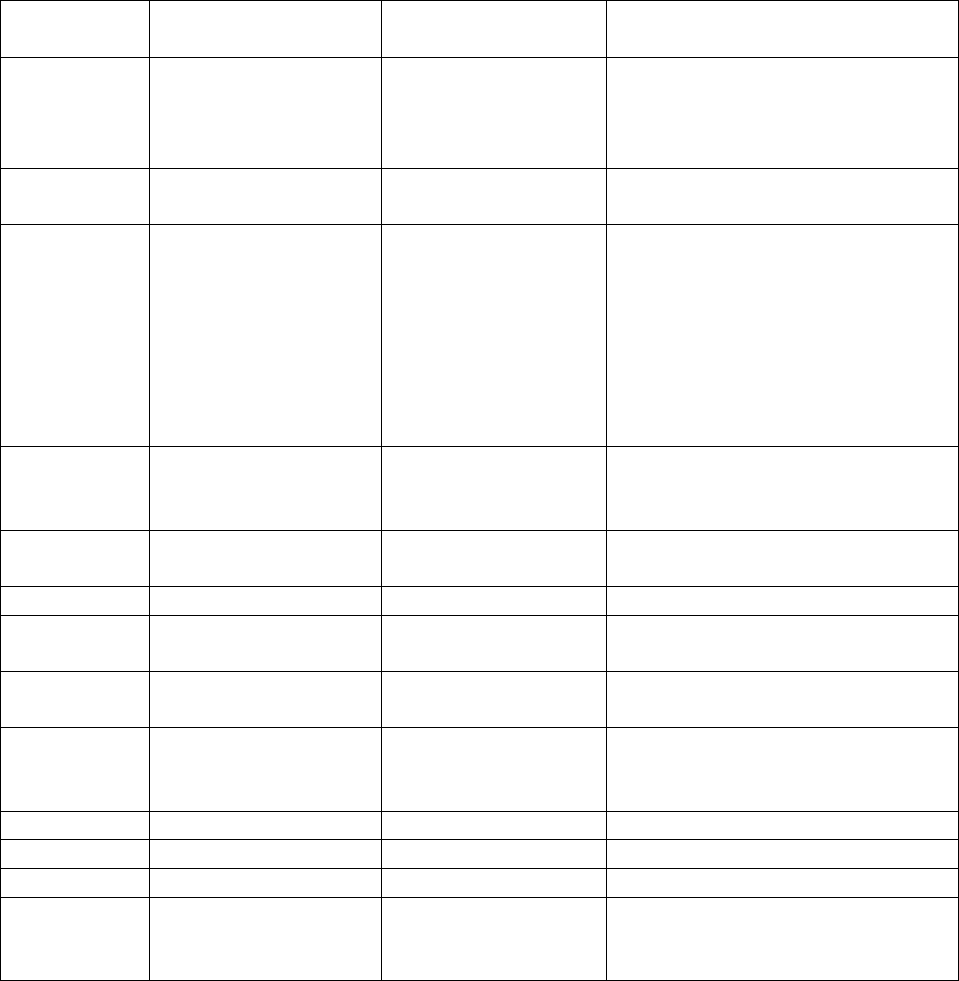
Program
County(ies)
Activities
Impact
Oral Disease and
Injury Prevention
Program (ODIP)
Funding: $781,907
Allegany, Anne
Arundel,
Baltimore,
Baltimore City,
Caroline, Carroll,
Cecil, Charles,
Dorchester,
Frederick, Garrett,
Harford, Howard,
Kent,
Montgomery,
Prince George’s,
Queen Anne’s, St.
Mary’s, Worcester
ODIP funds a variety of activities
aimed at supporting LHDs in
improving oral health conditions
through utilizing numerous strategies,
including:
- On-site clinical services for children;
- On-site clinical services for adults;
- Off-site oral health programs;
- School-based/linked community oral
health services;
- WIC (Supplemental Nutrition
Program for Women, Infants, and
Children) oral health services;
- Off-site oral cancer programs; and
- Off-site adult case management.
Children seen:
• In-clinic: 20,421
• In schools: 11,696
WIC patients screened: 5,837
Adults seen: 15,042
Dental Sealants
Program
Funding: $464,020
Allegany,
Baltimore, Calvert,
Cecil, Charles,
Harford, Kent,
Prince George’s,
Somerset,
Wicomico,
Worcester
The Dental Sealants program strives to
improve oral health conditions for
children through supporting school-
based, school-linked, and mobile
programs which:
- Screen children;
- Provide sealants; and
- Refer children for follow-up care.
Schools visited: 116
Children:
• Seen: 7,868
• Receiving sealants: 3,650
Sealants placed: 11,871
Deamonte Driver
Mobile Dental Van
Project
Funding: $120,000
Prince George’s
A Dental Sealants program, the
Deamonte Driver Mobile Dental
project is Prince George’s County’s
initiative which uses a mobile program
to screen children, provide sealants,
and refer children for follow-up care.
Schools visited: 7
Children:
• Seen: 226
• Receiving sealants: 162
Sealants placed: 599
Calvert Health
Systems
Funding: $130,000
Calvert, St. Mary’s
Calvert Health Systems provides
affordable and accessible oral health
care to children and adults. The
program provides funding for dental
care to those who cannot afford it but
require emergency intervention due to
severe abscess or decay. Additionally,
Calvert Health Systems continues to
partner with the Southern Maryland
Mission of Mercy and Tri-County
Veterans Council to host a Mission of
Mercy event for veterans and provide
follow-up care.
Children seen:
• In-clinic: 215
• In schools: 408
Adults seen: 1,281
2018 Annual Oral Health Legislative Report
Page 7
Program
County(ies)
Activities
Impact
Monocacy Health
Partners (MHP)
Funding: $50,000
Frederick
The MHP Dental Clinic offers dental
services to uninsured, underinsured,
and low-income residents.
Adults:
• Seen: 1,301
• Receiving emergency
treatment: 573
Maryland
Foundation of
Dentistry for the
Handicapped
Funding: $60,000
All counties
The Maryland Foundation of Dentistry
for the Handicapped is a 501(c) (3)
non-profit organization which recruits
volunteer dentists and specialists to
treat and educate patients and assist
patients with necessary case
management services.
Adults seen: 797
Federally-Funded Grant Projects
Hypertension Screening in the Dental Setting
OOH collaborated with the Department’s Center for Chronic Disease Prevention and Control
(CCDPC) to develop and implement the Models of Collaboration for State Chronic Disease and
Oral Health grant, funded by the Centers for Disease Control and Prevention (CDC), from 2016
through 2018. This collaboration created a program engaging dentists to provide hypertension
screenings during routine dental visits and, if necessary, provide patient referrals to primary care
providers for appropriate medical follow-up.
OOH and CCDPC collaborated with 14 LHDs throughout Maryland to implement program
activities. OOH and CCDPC staff trained LHD representatives using a “Train the Trainer”
approach. Once trained, LHD staff recruited dental practices and provided program training and
resources for dental staff to perform hypertension screenings. Over the two-year grant period, 47
dental practices participated and screened 36,996 individuals for hypertension. In addition, 2,689
individuals with undiagnosed or uncontrolled hypertension were referred to primary care
providers for further treatment. This collaboration aided in the effort to reduce the prevalence of
undiagnosed and uncontrolled hypertension among Maryland residents.
To promote hypertension screenings in the dental setting, OOH developed, produced, and
implemented a comprehensive statewide social marketing campaign entitled “Two Minutes with
Your Dentist Can Save Your Life.” The campaign educates Marylanders about the importance of
dentists in identifying undiagnosed hypertension and reminds dentists of the vital role they play
in each patient’s overall health. The campaign was communicated to the public through video
advertising in movie theaters and on gas station pump TV screens, as well as on social media
advertising on Facebook and other internet sites. In addition, materials such as posters, postcards,
and prescription pads were distributed to dental practices to help dentists educate their patients.
Spanish-Language Benefits and Safety of Tap Water Campaign
With funding from the Health Resources and Services Administration (HRSA), OOH developed
messaging for radio advertising, tested the messaging with focus groups of Latinas, produced

2018 Annual Oral Health Legislative Report
Page 8
radio advertisements, and launched a Spanish-language radio advertising campaign to promote
the safety and benefits of drinking tap water. The advertising message used a Spanish-speaking
dentist to discuss the safety and benefits of drinking tap water in Maryland, highlighting that tap
water contains fluoride, which protects teeth and prevents cavities. The campaign targeted
Latinas aged 18 to 45 in Baltimore, Howard, Montgomery, and Prince George’s Counties, and in
Baltimore City. Advertising ran on WLZL radio, Maryland’s largest and most popular Spanish-
language radio station. Advertisements also targeted Latinas on Pandora radio, YouTube, and
Facebook. The campaign ran in July and August of 2018. The 187,850 advertisements that ran
garnered almost 700,000 gross media impressions.
Perinatal and Infant Oral Health Quality Improvement Project
The Perinatal and Infant Oral Health Quality Improvement (PIOHQI) project, funded by HRSA's
Maternal and Child Health Bureau, spans from August 2015 to July 2019 and aims to reduce the
prevalence of oral disease in pregnant women and infants through improved access to high-
quality oral health care. In CY 2017, the University of Maryland College Park School of Public
Health, a contracted PlOHQI partner, conducted surveys, interviews, and focus groups of
pregnant women, personnel from the WIC program, and medical and dental providers to assess
barriers and facilitators to oral health care during pregnancy. Findings informed the development
of oral health educational materials, including a State guidance document on oral health care
during pregnancy, which was disseminated statewide to all dental and prenatal providers in May
2018. The guidance also serves to improve oral health integration into prenatal care and to
encourage dental providers to see women throughout the entire duration of pregnancy. The
PIOHQI project has several pilot prenatal sites involved in oral health care integration and
referral efforts, including LHD, FQHC, and hospital settings. The PIOHQI project also works
with home visiting programs in the State, in partnership with the Department’s Maternal, Infant,
and Early Childhood Home Visiting Program to integrate oral health into routine home visits
with families.
Expanding Oral Health Infrastructure
Maryland Oral Health Plan
In January 2018, the Maryland Dental Action Coalition (MDAC) released the updated Maryland
Oral Health Plan (MOHP), a five-year roadmap to improved oral health.
3
Funded by OOH, the
plan builds on oral health improvements achieved since the release of the first State plan in 2011,
identifies critical remaining gaps, and outlines strategies to improve the oral health and overall
health of Marylanders.
Statewide Summit
In June 2018, more than 120 representatives from a broad cross-section of oral health
stakeholders, including government, non-profits, clinical care providers, MCOs, associations,
foundations, and academia attended MDAC's Oral Health and Overall Health: Outcomes for
3
Maryland Oral Health Plan, 20189-2023. http://www.mdac.us/2018_01_14/MD_OHP_2018_0102.pdf

2018 Annual Oral Health Legislative Report
Page 9
Continued Success in Maryland statewide convening, funded by OOH and the DentaQuest
Foundation. In presentations focused on three key priorities of the updated MOHP, expert
speakers and panelists discussed health behaviors of the immigrant and Latino communities, the
impact of the uninsured on the public health system, cross-professional collaboration, the role of
community health workers, and racial disparities in oral health. Representatives from Medicaid
outlined the Department’s §1115 waiver application to the Centers for Medicare and Medicaid
Services (CMS) to establish a statewide Medicaid adult dental pilot program. Convening
attendees participated in a facilitated discussion on implementation of the pilot, and MDAC
submitted its input to Medicaid the following day.
Training of Dental and Medical Providers
On December 1, 2017, the eighth annual Ava Roberts Advanced Pediatric Dentistry Seminar
took place. The seminar was sponsored by OOH in collaboration with MDAC and the University
of Maryland School of Dentistry, with 128 individuals in attendance.
Community Water Fluoridation
Leading public health agencies, including the CDC and World Health Organization, endorse
community water fluoridation as the single most effective public health measure to improve oral
health by preventing tooth decay. Maryland has surpassed the Healthy People 2020 objective of
79.6 percent of the population with public water receiving fluoridated water, as 94.7 percent of
Marylanders with public water receive fluoridated water.
4
To address water fluoridation needs in
Maryland, OOH partners with the Maryland Department of the Environment (MDE) to create
fluoridation plans, share fluoridation data, monitor fluoride levels, and generate annual reports.
OOH continued to partner with the Maryland Rural Water Association to survey community
water systems and provide technical assistance. Twenty-four fluoridation stations across 20
water systems were surveyed in SFY 2018. The surveys highlighted both the continued need for
fluoridation equipment maintenance, repair, and replacement as well as the need for fluoridation
training for water operators. Through funding available from its CDC grant, OOH continues to
provide replacement fluoridation equipment to systems in need.
Maryland Community Health Resources Commission Dental Grant Awards
The Maryland Community Health Resources Commission (MCHRC) continues to partner with
OOH to expand and create new capacity for oral health care to serve low-income, underinsured,
and uninsured Marylanders. Since March 2008, MCHRC has awarded 39 dental services grants
totaling $7.8 million. The MCHRC dental grant projects, awarded to LHDs, FQHCs, and private
and non-profit foundations and hospitals, have collectively served approximately 62,000 low-
income children and adults, resulting in more than 136,000 visits.
MCHRC seeks to support programs that will be sustainable after initial grant funds have been
expended. The following is a summary of the grants awarded by the MCHRC in 2018.
4
Department of Health and Human Services, Healthy People 2020, Topics and Objectives,
http://www.healthypeople.gov/2020/topicsobjectives2020/objectiveslist.aspx?topicId=32, 5 October 2015.

2018 Annual Oral Health Legislative Report
Page 10
• Choptank Community Health Systems Inc. received a two-year grant ($240,000) to
address pediatric dental workforce challenges on the Eastern Shore by expanding access
to a new dental practice in Denton. Through a partnership with the University of
Maryland School of Dentistry, Choptank recruited a dental fellow to provide pediatric
dental services in their existing clinics in Federalsburg, Goldsboro, and Cambridge.
• Greater Baden Medical Services Inc. received a two-year grant ($300,000) to increase
access to dental care and nutritional counseling for low-income adults in Prince George’s
County. The project collaborates with Lyft to provide rides to appointments for residents
lacking access to transportation.
• Western Maryland Area Health Education Center received a two-year grant
($70,000) to expand an existing successful dental program that serves two jurisdictions
(Allegany and Garrett Counties) into a third jurisdiction (Washington County). The
program provides access to reduced price dentures for low-income residents who face
barriers accessing health and dental care.
Eastern Shore Oral Health Outreach Program
The OOH Lower Eastern Shore Oral Health Outreach Program provides seven Early Head Start
and Head Start Centers with oral health screenings, fluoride varnish applications, oral health
education, and case management. During the 2017-2018 school year, OOH screened 458 Head
Start students and 115 Early Head Start students. Each student was screened three times
throughout the school year, culminating in a total of 1,265 Head Start screenings and 398 Early
Head Start screenings.
5
For those students identified as presenting early evidence of cavities,
evidence of dental problems, or needing urgent care, the staff manages cases by referring the
students and their parents to dental clinics. Early Head Start and Head Start students started the
2017-2018 school year with a collective 49 percent needing case management services and
ended the school year with 45 percent needing case management services.
Maryland’s Mouths Matter: Fluoride Varnish and Oral Health Screening Program for Kids
In July 2009, the Department began training and reimbursing Medicaid Early and Periodic
Screening, Diagnosis, and Treatment Program (EPSDT) medical providers for the application of
fluoride varnish for children up to three years of age. Effective January 1, 2018, the new age
eligibility for the Maryland’s Mouths Matter program was nine months through age five. By
June 2018, 513 unique EPSDT-certified medical providers had administered 234,670 fluoride
varnish treatments to Medicaid children.
Maryland Dent-Care Loan Assistance Repayment Program
The purpose of the Maryland Dent-Care Loan Assistance Repayment Program (MDC-LARP) is
to improve access to oral health care by increasing the number of dentists that provide services to
Medicaid recipients. In January 2018, five new MDC-LARP dentists started their three-year
5
Early Head Start students received an additional screening in the summer; however, data for the fourth visit had
not yet been received at the time of this report’s completion.

2018 Annual Oral Health Legislative Report
Page 11
commitment to the program. During CY 2017, MDC-LARP dentists treated 24,188 unique
Medicaid patients and provided 60,471 dental visits for Medicaid recipients.
Oral Cancer Awareness Month
In April 2018, the Department observed Maryland Oral Cancer Awareness Month. OOH made
information available online to county coordinators, including prevention materials, scripts for
public service announcements, Maryland Tobacco Quitline resources, and articles for local
newspapers. The information addressed only oral cancer and the importance of the Human
Papillomavirus (HPV) vaccine which, in addition to preventing cervical cancer, can prevent
certain types of oral cancers.
Oral Cancer Initiative
Chapters 307 and 308 of the Acts of 2000 (HB 1184/SB 791) established the Department’s Oral
Cancer Initiative (Health-General Article, §18-801 and §18-802, Annotated Code of Maryland).
The major components of this initiative are oral cancer education for the public, education and
training for dental and non-dental health care providers, screening and referral if needed, and
evaluation of the program. The statute further requires OOH to develop activities and strategies
to prevent and detect oral cancer, with an emphasis on high-risk, underserved populations.
6
The
Oral Cancer Initiative funds the Oral Cancer Mortality Prevention Initiative. This initiative is
directed by OOH and provides grants to LHDs throughout Maryland to implement oral cancer
prevention initiatives, including oral cancer education and screenings for the public as well as
education and training for health care providers on how to conduct an oral cancer exam. In SFY
2018, 1,422 individuals received oral cancer screenings. Of those screened, 12 were referred to a
surgeon for a biopsy. Over 1,800 parents and caregivers were educated on HPV, a known cause
of oral cancer. Additionally, 95 health care providers received education on oral cancer.
In 2000, the Maryland General Assembly created the Cigarette Restitution Fund (CRF) Program
that provides funds for cancer prevention, education, screening, and treatment services for seven
targeted cancers, including oral cancer.
7
Some local jurisdictions provide oral cancer screening
and education and outreach services to residents. To date, CRF grants have funded oral cancer
prevention and early detection education, outreach and training services for 312,416 health care
providers, trainers and educators, and the public, resulting in 12,050 oral screening exams for
patients. In cooperation with OOH, the CRF Program is responsible for maintaining up-to-date
Oral Cancer Minimal Clinical Elements for screening, diagnosis, treatment, follow-up, and care
coordination services to provide guidance for public health programs that screen for oral cancer.
In addition, Johns Hopkins University and the University of Maryland use CRF cancer research
funds to conduct oral cancer research.
Part 2. Medicaid Dental Care Access
6
Md. Health General Code Ann. § 18-801.
7
Chapters 17 and 18 of the Acts of 2000 (SB 896/HB 1425), Md. Ann. Code Health-General Art., Title 13, Subtitles
10 and 11.

2018 Annual Oral Health Legislative Report
Page 12
The Maryland Medicaid program covers dental benefits through the Maryland Healthy Smiles
Dental Program. Dental services are covered for children aged 20 and younger under EPSDT,
pregnant women, certain adult populations, and former foster care youth until they become 26.
Non-pregnant adults may receive dental benefits provided as an additional benefit of their MCO.
As of July 2018, all nine MCOs voluntarily cover limited adult dental services to their members
as a part of their benefit package using their own profits. In addition, the Department is in the
process of implementing an adult dental pilot for adults aged 21 through 64 who are enrolled in
both Medicaid and Medicare.
Medicaid dental reimbursement for services for children, pregnant women, and participants
enrolled in the Rare and Expensive Case Management (REM) program has increased in recent
years to $186.8 million for CY 2017 (see Appendix B). The Medicaid program delivered oral
health services to 485,201 children and adults (ages 0-64) during CY 2017 compared to 463,964
in calendar year (CY) 2016; this is approximately a five-percent increase consistent with
Medicaid’s enrollment growth of five percent. Maryland continues to improve its dental program
by confronting barriers to providing comprehensive oral health services to Medicaid participants.
Availability and Accessibility of Dentists in Medicaid
Since 2009, a single statewide dental ASO has overseen services for Maryland Healthy Smiles
Dental Program participants. Scion currently serves as the ASO. The ASO is responsible for
credentialing, billing, and dental provider issues, which streamlines the process for providers. As
a result, the Department has been able to increase the Medicaid dental provider network. The
Dental Home Program was implemented statewide in December 2013.
With the goal of increasing dental provider enrollment, the Department outlined pay-for-
performance standards in the February 2015 in the Maryland Medicaid Dental Benefits
Administrator Request for Proposals. The pay-for-performance standards incentivize provider
outreach and reward the ASO for increasing provider enrollment in target counties. The ASO
must be able to demonstrate improvement across two ratios: 1) the general dentist provider-to-
participant ratio and 2) the dental specialist provider-to-patient ratio.
8
Performance payments are
tiered and allow for continued demonstrations of improvement over the life of the contract. In
CY 2016 and CY 2017, Scion added 140 access points as part of this incentive: 11 endodontists,
99 general dentists, six oral surgeons, eight orthodontists, and 16 pediatric dentists. Scion will
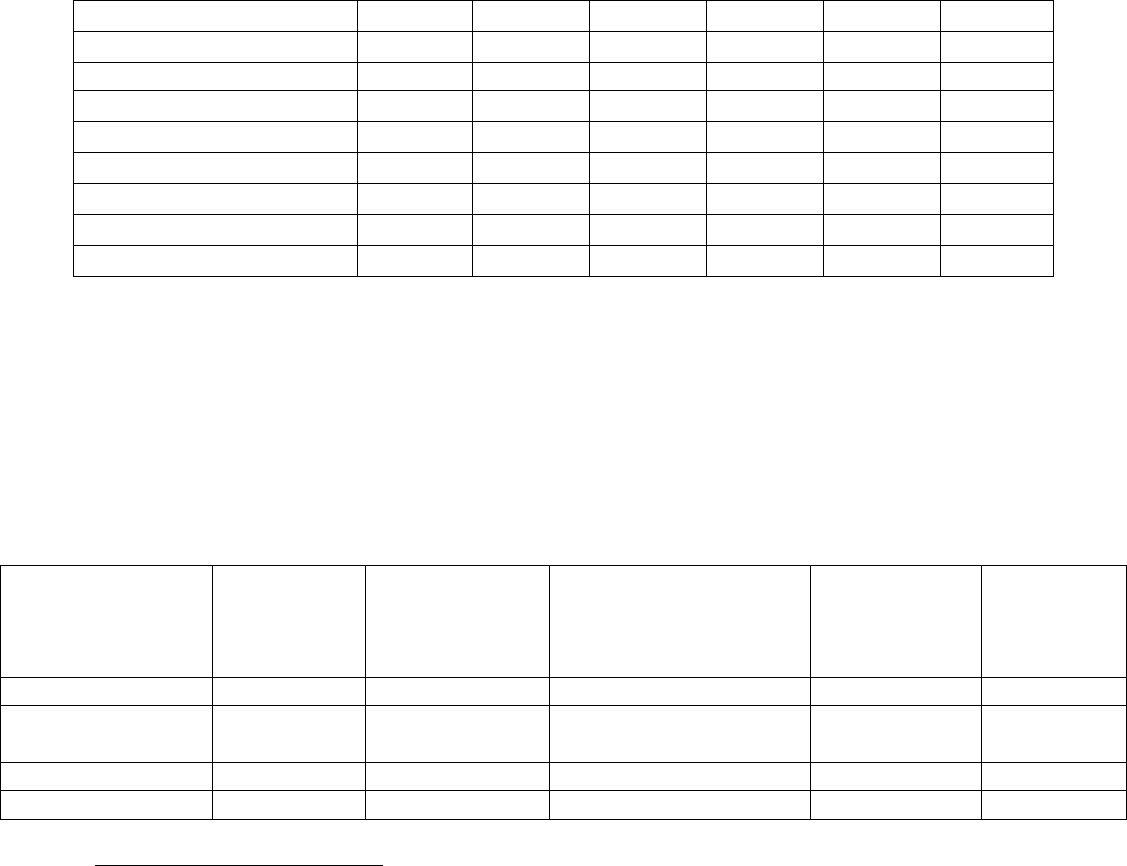
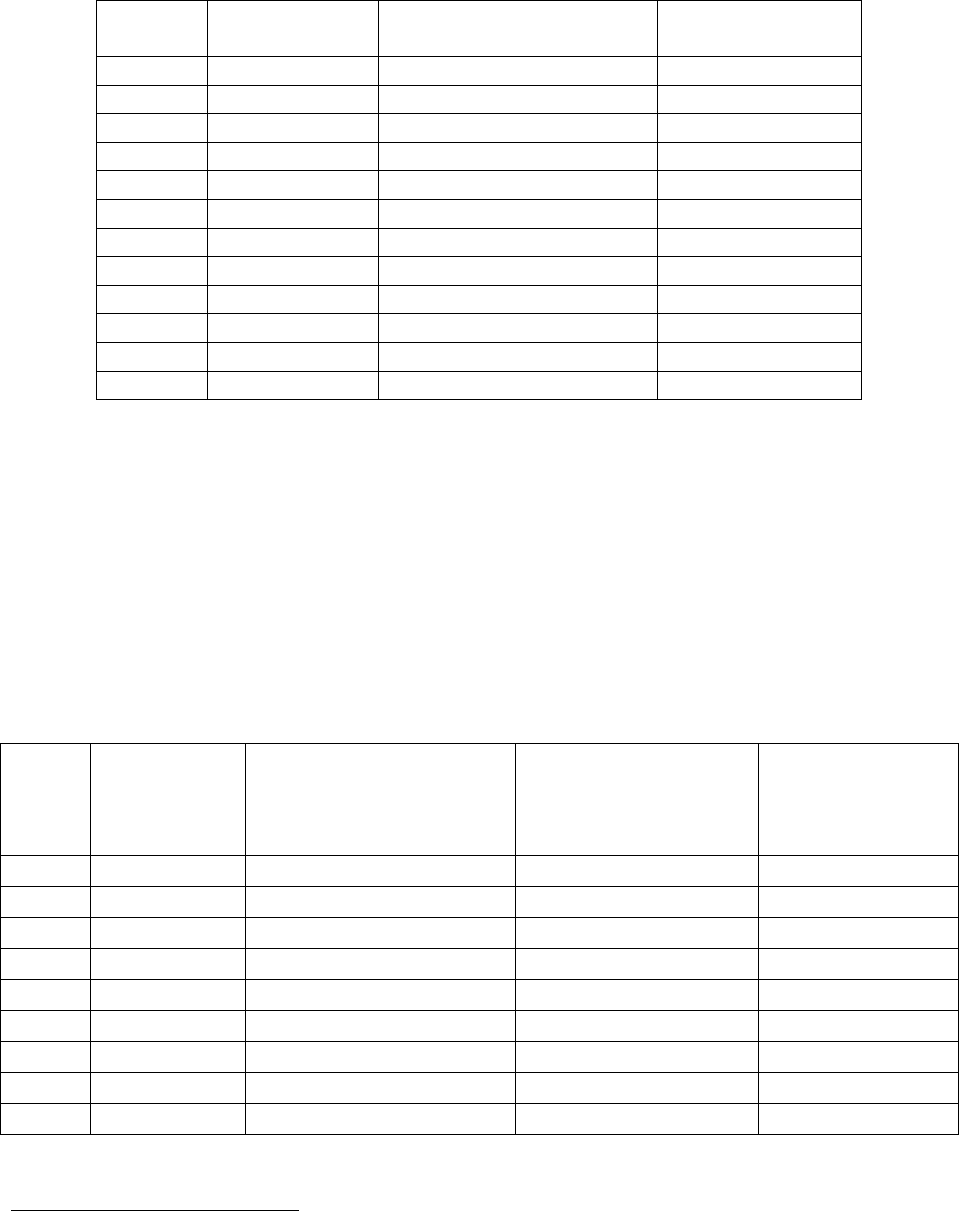
continue outreach to dental providers to increase participation in the program. In CY 2017, there
were 1,625 total (1,600 unique) providers enrolled (see Table 2).
Table 2: Number of Dentists Participating in Medicaid who Billed One or More Services,
by Region
8
The ASO is tasked with demonstrating improvement in counties that were not meeting the 1:500 general dentist
provider-to-participant ratio and the 1:10,000 dental specialists provider-to-patient ratio as of January 1, 2016.
2018 Annual Oral Health Legislative Report
Page 13
Region
9
CY 2012
CY 2013
CY 2014
CY 2015
CY 2016
CY 2017
Baltimore Metro
465
471
490
536
538
560
Washington, D.C. Suburbs
451
462
525
564
567
563
Southern Maryland
52
48
55
54
60
63
Western Maryland
126
124
117
128
122
145
Eastern Shore
72
84
84
89
86
97
Out-of-State
125
161
179
182
167
197
Total
10
1,291
1,350
1,450
1,464
1,540
1,625
Unique Total
11
1,220
1,258
1,361
1,470
1,467
1,600
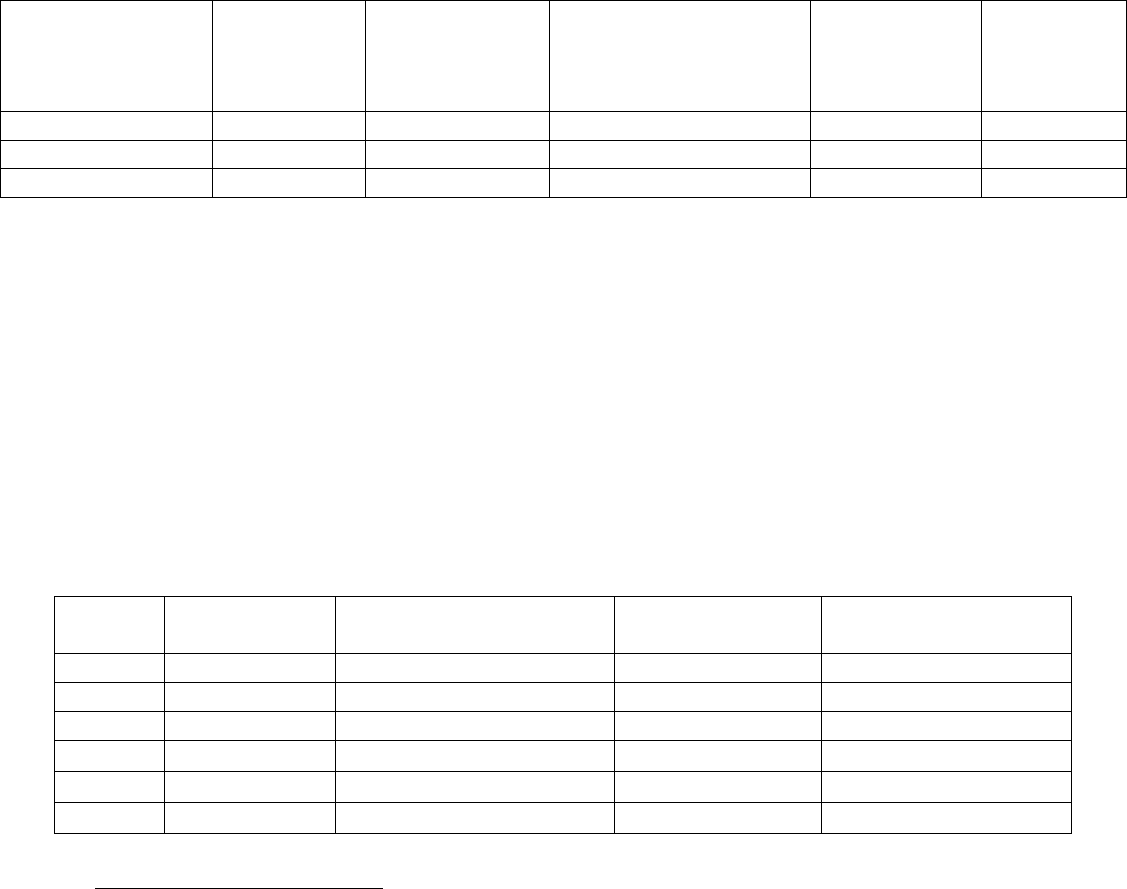
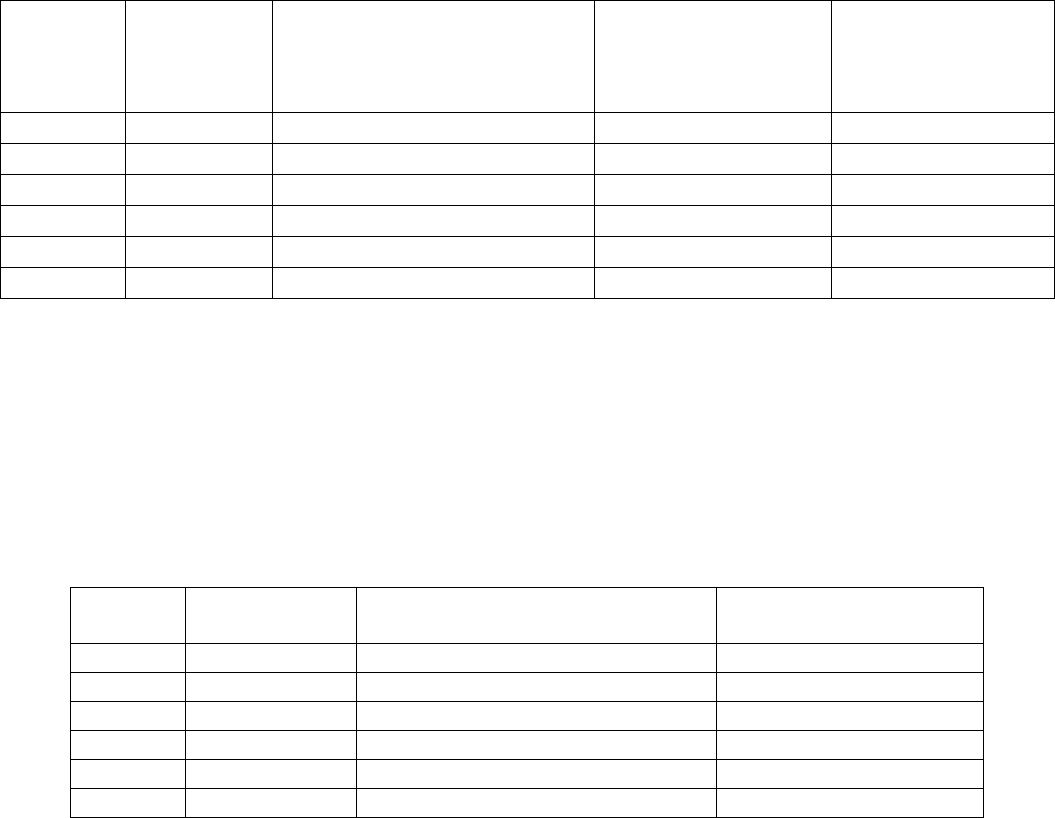
According to the Maryland State Board of Dental Examiners, there were 4,014 dentists actively
practicing in Maryland in August 2018 (see Table 3). As of August 2018, 1,521 dentists
participated with the Maryland Healthy Smiles Dental Program. In CY 2017, 1,600 unduplicated
dentists billed one or more Medicaid services, and 1,255 unduplicated dentists billed $10,000 or
more to the Medicaid program. This represents approximately 39.9 percent and 31.3 percent
respectively of the total active, licensed dentists in the state.
Table 3: Active Dentists and Dentists Participating with the Maryland Healthy Smiles
Dental Program
Region
Total Active
Dentists
(August
2018)
12
Active
Pediatric
Dentists
(August 2018)
13
Dentists Enrolled with
Maryland Healthy
Smiles Dental Program
(August 2018)
14
Dentists Who
Billed One or
More Services
in CY 2017
15
Dentists
Who Billed
$10,000+ in
CY 2017
16
Baltimore Metro
1,735
56
642
560
454
Washington D.C.
Suburbs
1,624
53
667
563
472
Southern Maryland
157
6
88
63
53
Western Maryland
278
8
200
145
116
9
Baltimore Metro includes Baltimore City and Anne Arundel, Baltimore, Carroll, Harford, and Howard Counties.
Washington, D.C. suburbs include Prince George’s and Montgomery Counties. Southern Maryland includes Calvert,
Charles, and St. Mary’s Counties. Western Maryland includes Allegany, Frederick, Garrett, and Washington
Counties. The Eastern Shore includes Caroline, Cecil, Dorchester, Kent, Queen Anne’s, Somerset, Talbot,
Wicomico, and Worcester Counties.
10
Please note that the total is the sum of all regions.
11
Please note that the unique total does not equal the sum of all regions because an individual dentist may have
offices in multiple regions. The unique total reflects the number of unique dentists unduplicated statewide. This
unique total also includes out-of-state dentists who served Maryland Medicaid enrollees.
12
Source: Maryland Board of Dental Examiners
13
Source: Ibid
14
Source: Scion
15
Records were manually unduplicated by provider name because providers who practice in multiple locations may
have different provider numbers for each practice affiliation. Dentists working for group practices or clinics were
impossible to identify; therefore, the number of unique providers may significantly undercount the total number of
dentists providing dental services to Medicaid enrollees.
16
See previous footnote.
2018 Annual Oral Health Legislative Report
Page 14
Region
Total Active
Dentists
(August
2018)
12
Active
Pediatric
Dentists
(August 2018)
13
Dentists Enrolled with
Maryland Healthy
Smiles Dental Program
(August 2018)
14
Dentists Who
Billed One or
More Services
in CY 2017
15
Dentists
Who Billed
$10,000+ in
CY 2017
16
Eastern Shore
220
6
161
97
82
Out-of-State
--
--
222
197
79
TOTAL
17
4,014
129
1,521
1,600
1,255
Maryland Healthy Smiles Dental Program Dental Utilization Rates
Children and Dental Utilization
Under EPSDT requirements, dental care is a mandated health benefit for children under 21 years
of age.
18
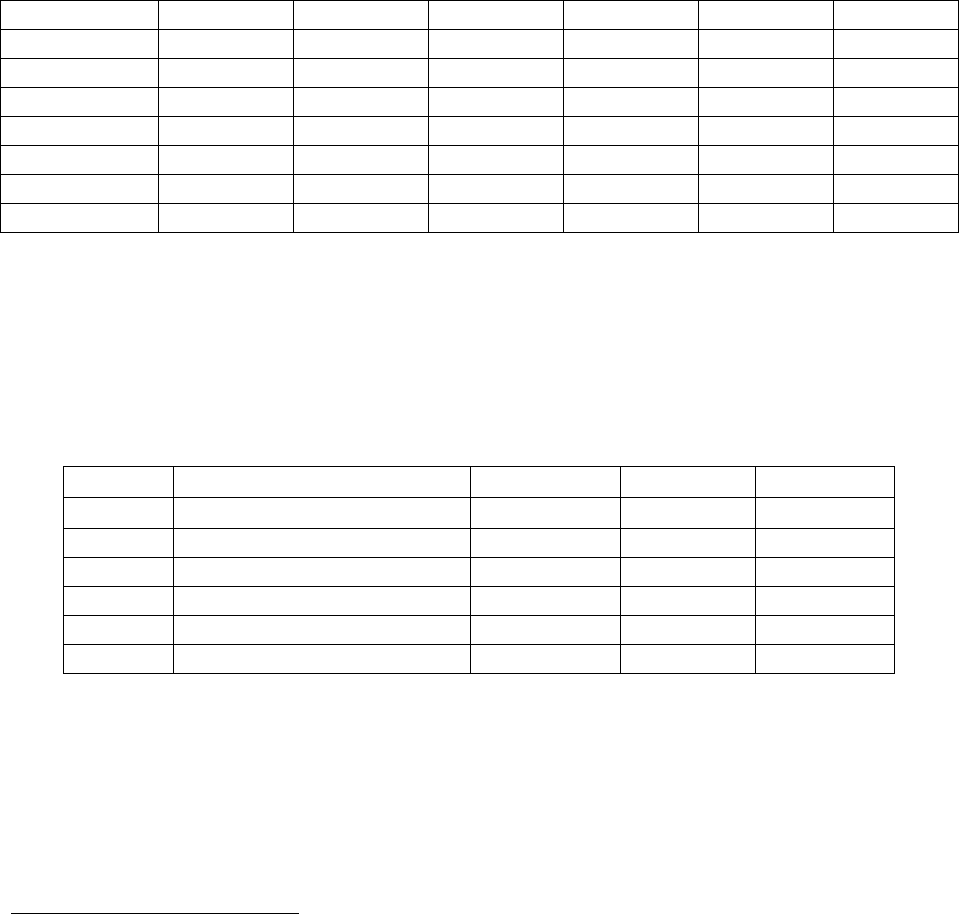
To assess the performance of HealthChoice and the ASO, Medicaid uses a measure
closely modeled after the National Committee for Quality Assurance Healthcare Effectiveness
Data and Information Set (HEDIS®) measure for Medicaid children’s dental services utilization.
In CY 2017, 68.1 percent of children received dental services, which is greater than the national
HEDIS® mean (see Table 4).
Table 4: Number of Children Aged 4-20 Years Enrolled in Medicaid
19
for at least 320 Days
Receiving Dental Services, CY 2012 - CY 2017
Year
Total Number
of Enrollees
Enrollees Receiving One
or More Dental Services
Percent Receiving
Service
HEDIS® National
Medicaid Average
20,21
CY 2012
385,132
261,077
67.8%
49.2%
CY 2013
405,873
277,272
68.3%
↑
CY 2014
423,625
286,713
67.7%
↑
CY 2015
404,118
278,796
69.0%
↑
CY 2016
440,100
301,367
68.5%
↑
CY 2017
464,585
316,294
68.1%
↑
17
Please note that the totals for Maryland Healthy Smiles Dental Program enrollment, dentists billing one or more
services, and dentists billing more than $10,000 in services do not equal the sum of all regions because an individual
dentist may have offices in multiple regions. The totals listed reflect the number of unique dentists unduplicated
statewide for CY 2016.
18
Children are only covered up to age 19 under the Maryland Children’s Health Program and up to age 20 under
Medicaid.
19
The study population for CY 2012 through CY 2016 measured dental utilization for all qualifying individuals in
Maryland’s Medicaid program, including fee-for service (FFS) and HealthChoice MCO enrollees. The following
coverage groups were excluded from the analysis: S09, X02, W01, and P10. Recipients with partial benefits were
also excluded from the analysis.
20
Mean for the Annual Dental Visit measure, total age category (ages 2-21 years), as of HEDIS® 2006. The 2-3
year age cohort was added as of HEDIS® 2006.
21
Due to National Committee for Quality Assurance licensing restrictions beginning with CY 2013, the National
HEDIS® Mean can no longer be displayed in Table 4. An arrow has been added to indicate if Maryland’s
performance score is above, below, or equal to the National HEDIS® Mean. In CY 2013, CY 2014, CY 2015, and
2016, Maryland’s performance score was above the National HEDIS® Mean.
2018 Annual Oral Health Legislative Report
Page 15
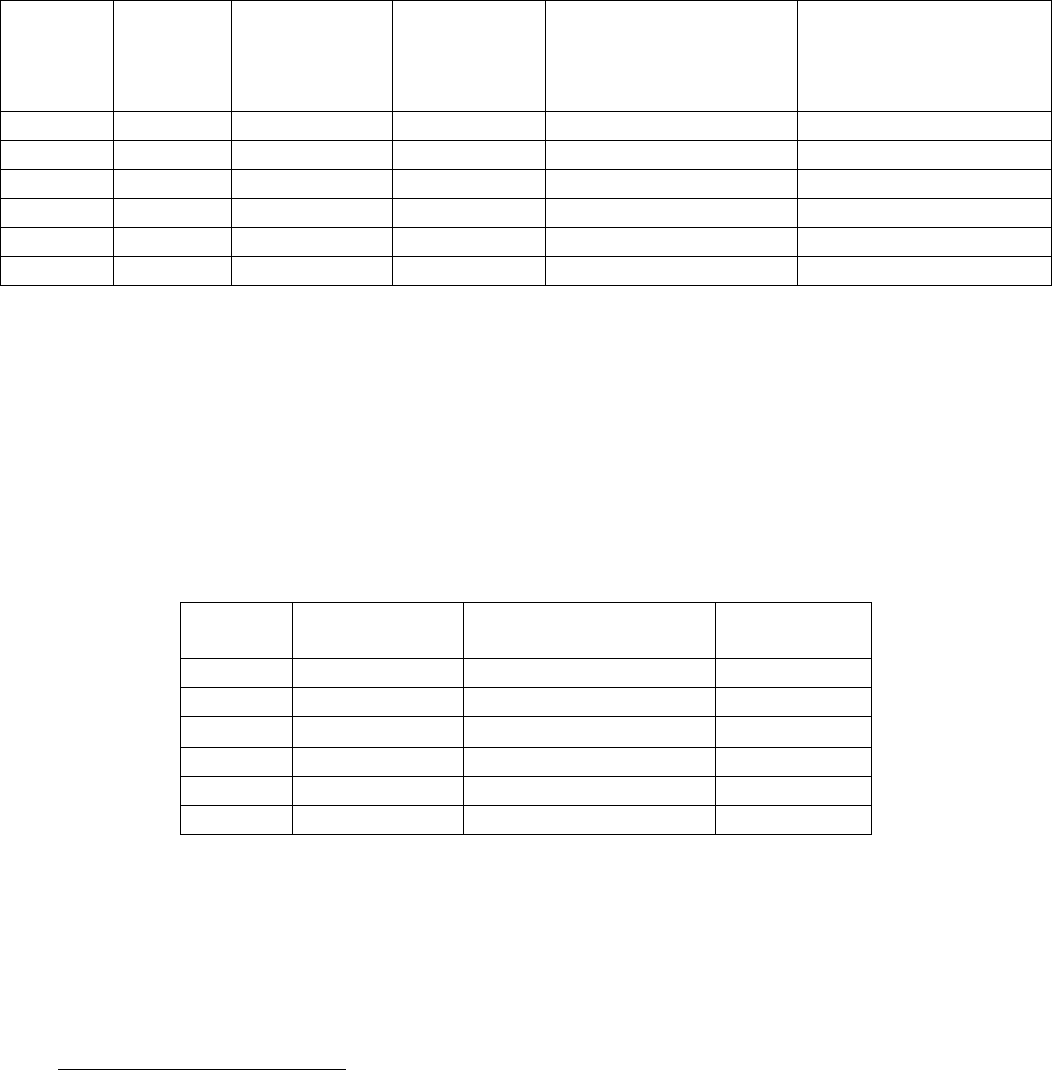
Of the 723,709 children enrolled in Medicaid for any period during CY 2017, 55.0 percent of
these children received one or more dental service compared to 54.5 percent in CY 2016 (see
Table 5). The utilization rates of children with any period of enrollment have increased over the
five-year period for all age groups.
Table 5: Percentage of Children Aged 0–20 Years Enrolled in Medicaid
22
for Any Period
who Had at Least One Dental Visit by Age Group, CY 2012 - CY 2017
Age Group
CY 2012
CY 2013
CY 2014
CY 2015
CY 2016
CY 2017
0–3
27.9%
29.8%
29.8%
28.9%
30.0%
30.3%
4–5
64.8%
65.8%
65.2%
64.7%
66.3%
65.8%
6–9
67.8%
68.9%
68.0%
68.0%
69.1%
69.2%
10–14
62.9%
63.4%
62.1%
62.8%
64.7%
65.6%
15–18
52.4%
53.2%
51.3%
51.6%
54.3%
55.6%
19–20
35.1%
35.8%
34.3%
34.0%
36.7%
37.3%
All
52.3%
53.7%
52.9%
52.8%
54.5%
55.0%
In response to the concern that the level of restorative services or treatment may not be adequate,
Medicaid has examined the type of dental services that children receive. Utilization of diagnostic
services increased from 66 percent in CY 2012 to 66.5 percent in CY 2017, while utilization of
restorative services has decreased from approximately 24 percent of all children in CY 2012 to
23 percent in CY 2017 (see Table 6).
Table 6: Percentage of Children Aged 4-20 Years Enrolled in Medicaid
23
for at least 320
Days Receiving Dental Services, by Type of Service, CY 2012 - CY 2017
Year
Total Number of Enrollees
Diagnostic
Preventive
Restorative
CY 2012
385,132
66.0%
62.5%
24.3%
CY 2013
405,873
66.8%
63.2%
24.4%
CY 2014
423,625
66.2%
62.6%
23.2%
CY 2015
404,118
67.6%
64.0%
24.0%
CY 2016
440,100
67.0%
63.4%
23.2%
CY 2017
464,585
66.5%
62.9%
23.2%
Utilization rates are lower when analyzed for any period of enrollment versus a period of
continuous enrollment, because the MCO or ASO has had less opportunity to manage the care of
these populations. For those children enrolled in Medicaid for any period, 54.2 percent received
a preventive or diagnostic visit in CY 2017. Of those receiving a preventive or diagnostic visit,
29.1 percent received a follow-up restorative visit (see Table 7).
22
The study population for CY 2012 through CY 2016 measured dental utilization for all qualifying individuals in
Maryland’s Medicaid program, including fee-for service (FFS) and HealthChoice MCO enrollees. The following
coverage groups were excluded from the analysis: S09, X02, W01, and P10.
23
The study population for CY 2012 through CY 2016 measured dental utilization for all qualifying individuals in
Maryland’s Medicaid program, including fee-for service (FFS) and HealthChoice MCO enrollees. The following
coverage groups were excluded from the analysis: S09, X02, W01, and P10.
2018 Annual Oral Health Legislative Report
Page 16
Table 7: Percentage of Children Aged 0–20 Years Enrolled in Medicaid
24
for Any Period
who Received a Preventive/Diagnostic Visit Followed by a Restorative Visit, CY 2012 - CY
2017
Year
Total
Number
of
Enrollees
Number with
Preventive/
Diagnostic
Visit
Percent with
Preventive/
Diagnostic
Visit
Number with
Preventive/ Diagnostic
Visit Followed by a
Restorative Visit
Percent with
Preventive/ Diagnostic
Visit Followed by a
Restorative Visit
CY 2012
645,562
331,496
51.3%
102,028
30.8%
CY 2013
661,872
349,864
52.9%
106,862
30.5%
CY 2014
706,378
367,908
52.1%
107,595
29.2%
CY 2015
709,669
369,645
52.1%
109,614
29.7%
CY 2016
702,105
377,058
53.7%
109,048
28.9%
CY 2017
723,709
391,897
54.2%
114,089
29.1%
Pregnant Women and Dental Utilization
Chapter 113 of the Acts of 1998 (SB 590) required that HealthChoice cover dental services for
all pregnant women. The percentage of pregnant women 21 years and over enrolled for at least
90 days receiving dental services was approximately 27 percent in CY 2017 (see Table 8).
Table 8: Number and Percentage of Pregnant Women Aged 21+ Years with at least 90
Days in Medicaid
25
who had Dental Services, CY 2012 - CY 2017
Year
Total Number
of Enrollees
Number of Enrollees
with at least One Visit
Percent with
Dental Visits
CY 2012
21,708
6,537
30.1%
CY 2013
22,286
6,113
27.4%
CY 2014
25,408
6,858
27.0%
CY 2015
26,795
7,324
27.3%
CY 2016
29,014
7,562
26.1%
CY 2017
29,111
7,981
27.4%
HealthChoice Dental Utilization Rates
Apart from dental services covered for pregnant women and adults in REM, adult dental services
are not covered under HealthChoice or the Maryland Healthy Smiles Dental Program. Prior to
the dental carve-out and implementation of the Dental ASO, all of the HealthChoice MCOs
24
Please see previous footnote.
25
The study population for CY 2012 through CY 2016 measured dental utilization for all qualifying individuals in
Maryland’s Medicaid program, including fee-for service (FFS) and HealthChoice MCO enrollees. The following
coverage groups were excluded from the analysis: S09, X02, W01, and P10.
2018 Annual Oral Health Legislative Report
Page 17
provided a limited adult dental benefit. As of July 2018, all nine HealthChoice MCOs provide
limited dental services to non-pregnant adults (see Table 9).
Table 9: HealthChoice Dental Benefits for Non-Pregnant Adults as of July 1, 2018
MCO
Dental Benefits Offered
Limitations Apply and Vary by MCO
Maximum Benefit Limit
per CY
Aetna Better Health
Oral exam, fluoride treatment, and cleaning twice a
year; x-rays; fillings; extractions; and emergency
palliative treatment (limit four per year)
$750 (not including basic
care such as exams and
cleanings)
Amerigroup
Community Care
Oral exam and cleaning twice a year; x-rays; fillings
and extractions
$250
Jai Medical Systems
Oral exam and cleaning twice a year; x-rays; fillings
and extractions
$500
Kaiser Permanente
Oral exam and cleaning twice a year; x-rays; fillings
and extractions
$750
Maryland Physicians
Care
Oral exam and cleaning twice a year; x-rays; fillings
and extractions
30% coinsurance for fillings
and extractions; 20% off
non-covered dental services
MedStar Family Choice
Oral exam and cleaning twice a year; x-rays; fillings
and extractions
None
Priority Partners
Oral exam and cleaning twice a year; x-rays and
extractions
None
University of Maryland
Health Partners
Oral exam and cleaning twice a year; x-rays; fillings
and extractions
$350
United Healthcare
Oral exam and cleaning twice a year; x-rays; fillings
and extractions
$250
Beginning January 1, 2014, Maryland expanded Medicaid eligibility to low-income families and
adults under age 65 under the Patient Protection and Affordable Care Act. Since then,
HealthChoice adult dental expenditures have risen because of the subsequent increased
enrollment. In CY 2017, adult HealthChoice enrollees increased to 569,948, of which 85,323
received at least one dental service through the MCOs’ value-added benefits. In CY 2017, 15.0
percent of non-pregnant adults enrolled in a HealthChoice MCO for at least 90 days received at
least one dental service, up from 13.9 percent in CY 2016 (see Table 10).
Table 10: Percentage of Non-Pregnant Adults 21-64 Receiving Dental Services, Enrolled in
HealthChoice for at Least 90 Days
Year
Total Number
of Enrollees
Enrollees Receiving One
or More Dental Service
Percent
Receiving Service
CY 2000
114,223
16,986
14.9%
CY 2001
111,694
16,795
15.0%
CY 2002
117,885
16,800
14.3%
CY 2003
116,880
21,288
18.2%
CY 2004
115,441
12,457
10.8%
CY 2005
116,266
11,093
9.5%
2018 Annual Oral Health Legislative Report
Page 18
Year
Total Number
of Enrollees
Enrollees Receiving One
or More Dental Service
Percent
Receiving Service
CY 2006
114,844
11,747
10.2%
CY 2007
138,212
18,290
13.2%
CY 2008
125,386
23,587
18.8%
CY 2009
177,474
26,063
14.7%
CY 2010
192,835
33,117
17.2%
CY 2011
222,580
50,652
22.8%
CY 2012
236,205
51,619
21.9%
CY 2013
248,524
33,093
13.3%
CY 2014
486,025
65,671
13.5%
CY 2015
533,689
72,556
13.6%
CY 2016
521,954
72,318
13.9%
CY 2017
569,948
85,323
15.0%
Emergency Department Utilization
In CY 2017, 20,255 children and adults with any period of enrollment in HealthChoice visited
the emergency department (ED) with a dental diagnosis, not including accidents, injury, or
poison (see Table 11). Of those, 17,600 adults aged 21 and older visited the ED with a dental
diagnosis, compared to 18,175 in CY 2016.
Table 11: Number and Percentage of Medicaid Participants Aged 0 - 64 years with at least
One ED Visit with a Dental Diagnosis or Dental Procedure Code, CY 2017
Age
Group
Total
Participants
Number of Participants
with ED Visit with
Dental Diagnosis or
Procedure
Percentage with ED
Visit with Dental
Diagnosis or
Procedure
Total Number of
Visits with
Dental Diagnosis
or Procedure
0 - 3
26
158,892
770
0.5%
1,304
4 - 5
74,865
248
0.3%
433
6 - 9
151,770
495
0.3%
861
10 - 14
170,502
314
0.2%
550
15 - 18
116,825
401
0.3%
787
19 - 20
50,855
427
0.8%
910
21 - 39
398,351
11,897
3.0%
29,911
40 - 64
340,815
5,703
1.7%
13,229
Total
1,462,875
20,255
1.4%
47,985
26
Most newborns and infants are not expected to use dental services. As a result, the dental service rate for the 0-3
age groups should be interpreted with caution.
2018 Annual Oral Health Legislative Report
Page 19
In CY 2017, the percent of participants with an ED visit with a dental diagnosis or procedure
decreased to 1.4 percent (see Table 12). In CY 2017, the total number of visits decreased to
47,985.
Table 12: Number and Percentage of Medicaid Participants Aged 0 - 64 years with at least
One ED Visit with a Dental Diagnosis or Dental Procedure Code, CY 2012 - CY 2017
Year
Total
Participants
Number of Participants with
ED Visit with
Dental Diagnosis or
Procedure
Percentage with
ED Visit with
Dental Diagnosis or
Procedure
Total Number of
Visits with Dental
Diagnosis or
Procedure
CY 2012
1,001,081
14,757
1.5%
38,421
CY 2013
1,031,029
15,093
1.5%
39,358
CY 2014
1,378,963
22,293
1.6%
57,679
CY 2015
1,437,496
21,227
1.5%
52,661
CY 2016
1,401,793
20,916
1.5%
51,168
CY 2017
1,462,875
20,255
1.4%
47,985
In CY 2016, 2,655 children with any period of enrollment in HealthChoice visited the ED with a
dental diagnosis, not including accidents, injury, or poison. The percentage of children with ED
visits relative to the total Medicaid population eligible for dental services continued to decline
across the five-year period and has remained at less than one percent.
Table 13: Number of ED Visits with a Dental Diagnosis or Procedure by Children Aged 0–
20 Years Enrolled in Medicaid for any Period, CY 2012 - CY 2017
Year
Total Number
of Enrollees
Number of Enrollees who had an
ED Visit with a Dental Diagnosis
Number of ED Visits
with a Dental Diagnosis
CY 2012
645,562
2,899
5,699
CY 2013
661,872
2,815
5,464
CY 2014
706,378
2,806
5,337
CY 2015
709,669
2,642
5,547
CY 2016
702,105
2,741
5,090
CY 2017
723,709
2,655
4,845
Recent Dental Legislation and Program Expansions
Expansion of Dental Services to Former Foster Care Youth
Chapters 57 and 58 of the Acts of 2016 (SB 252/HB 511) authorized Medicaid to cover dental
care for former foster care youth until they reach age 26, and required Medicaid to apply to CMS
for the necessary waiver to receive a federal match for these services. CMS granted Maryland a
waiver to cover these services, and Maryland has provided dental services as an EPSDT benefit
to former foster care youth since January 1, 2017.
2018 Annual Oral Health Legislative Report
Page 20
Proposed Adult Dental Pilot
On May 15, 2018, Governor Hogan signed SB 284 - Maryland Medical Assistance Program -
Dental Coverage for Adults - Pilot Program (Chapter 621 of the Acts of 2018) into law. The law
requires the Department to implement an adult dental pilot and to apply for a waiver from CMS
if necessary. The Department submitted an amendment to its §1115 waiver to CMS on July 2,
2018. Subject to the approval of CMS, the adult dental pilot program will go into effect in the
first half of 2019. As required in SB284, the objective in seeking this amendment is to determine
whether offering an adult dental benefit will improve health outcomes for vulnerable adults.
The proposed statewide pilot program will serve individuals between the ages of 21 and 64 who
are dually-eligible for both Medicare and Medicaid. The Department estimates approximately
38,510 participants will gain dental coverage under the pilot. Dually-eligible individuals do not
currently receive dental benefits through Medicaid, and coverage for dental services through
Medicare is extremely limited.
27
Based on analysis performed by the Hilltop Institute, the total
estimated cost of the program is $5.0 million. These costs are subject to a 50 percent federal
match; the total state share of the cost is approximately $2.5 million.
The proposed dental package includes coverage for diagnostic, preventive, and restorative
services, in addition to extractions. Benefits will be subject to an $800 per person cap per
calendar year for the first year of the pilot, which may be subject to review for subsequent
demonstration years. These benefits will be carved out and overseen by the dental ASO. A copy
of the Department’s §1115 waiver amendment to CMS, which includes a more extensive
discussion of the proposed pilot, can be found online at
https://mmcp.health.maryland.gov/Pages/1115-HealthChoice-Waiver-Renewal.aspx.
III. Conclusion and Future Initiatives
In 2019, the Department intends to increase the number of dental service providers; expand
education, prevention, and outreach initiatives; promote oral health literacy for the public; and
provide funding support for the Oral Cancer Initiative. It will work to increase the provision of
prevention, early intervention, and educational oral health services in high-risk, low-income
venues such as WIC, and Head Start/Early Head Start programs, as well as in Title I schools.
The Department greatly appreciates the strong commitment demonstrated by the Governor and
the Maryland General Assembly to transforming Maryland’s capacity to provide oral health
services.
27
Medicare does not cover most dental care, dental procedures, or supplies, such as cleanings, fillings, tooth
extractions, dentures, dental plates, or other dental devices. Medicare Part A pays for certain dental services that are
obtained when a Medicare participant is in a hospital.
2018 Annual Oral Health Legislative Report
Page 21
Appendix A: Glossary of Key Abbreviations
ASO
Administrative Services Organization
CY
Calendar Year
CCDPC
Center for Chronic Disease Control and Prevention
CDC
Centers for Disease Control and Prevention
CMS
Centers for Medicare and Medicaid Services
The
Department
Maryland Department of Health (formerly the Department of Health and Mental
Hygiene)
ED
Emergency Department
EPSDT
Early and Periodic Screening, Diagnosis, and Treatment Program
FFS
Fee-for-service
FQHC
Federally-Qualified Health Center
HB
House Bill
HPSA
Health Professional Shortage Area
HPV
Human Papillomavirus
HRSA
Health Resources and Services Administration
LHD
Local Health Department
MCO
Managed Care Organization
MCHRC
Maryland Community Health Resources Commission
MDAC
Maryland Dental Action Coalition
MDC-LARP
Maryland Dent-Care Loan Assistance Repayment Program
Medicaid
Maryland Medical Assistance Program
MOHP
Maryland Oral Health Plan
HEDIS®
National Committee for Quality Assurance Healthcare Effectiveness Data and
Information Set
OOH
Office of Oral Health
ODIP
Oral Disease and Injury Prevention Program
PIOHQI
Perinatal and Infant Oral Health Quality Improvement
SB
Senate Bill
Scion
Scion Dental, Inc.
SFY
State Fiscal Year
WIC
Supplemental Nutrition Program for Women, Infants and Children
2018 Annual Oral Health Legislative Report
Page 22
Appendix B: Medicaid Dental Funding, Expenditures, and Utilization Rates; MCO and
Maryland Healthy Smiles Dental Program Funding and Expenditures for Dental Services;
and Utilization of Dental Services in HealthChoice and DentaQuest, SFY 1997 - CY 2017
Year
Amount Paid in
MCO Capitation
Rates or
Maryland
Healthy Smiles
Dental Program
Amount
Spent by
MCOs for
Dental
±
(Includes
Adult Dental)
Utilization Rate for
General Access
(Children 4-20
Years with 320 Days
of Enrollment)
Utilization Rate for
Restorative
(Children 4-20
Years with 320 Days
of Enrollment)
SFY 1997
N/A
$2.7 M*
19.9%
6.6%
CY 2000
$12.3 M (est.)
$17 M (est.)
28.7%
9.3%
CY 2001
$27.1 M
$23.6 M
33.6%
10.8%
CY 2002
$40.3 M
$28.9 M
34.5%
10.3%
CY 2003
$33 M
$32.5 M
43.2%
13.6%
CY 2004
$28 M
$36.7 M
43.7%
13.8%
CY 2005
$33 M
$42.0 M
45.8%
15.8%
CY 2006
$35.1 M
$46.6 M
46.2%
16.4%
CY 2007
$42.5 M
$53.8 M
51.5%
19.3%
CY 2008
$55.4 M
$71.4 M
54.6%
†
20.8%
†
CY 2009**
$82.8 M
$39.6 M
60.9%
23.2%
CY 2010***
$137.6 M
$6.5 M
64.1%
25.1%
CY 2011
$152.7 M
$11.4 M
66.6%
25.2%
CY 2012
$150.5 M
$11.1 M
67.8%
24.3%
CY 2013
$157.2 M
$5.3 M
68.3%
24.4%
CY 2014
$159.0 M
$16.5 M
67.7%
23.2%
CY 2015
$165.2 M
$14.4 M
69.0%
24.0%
CY 2016
$174.6 M
$15.3 M
68.5%
23.2%
CY 2017
$186.8 M
$17.0 M
68.1%
23.2%
* In SFY 1997, the Department spent $2.7 M on dental services under its FFS program.
** In CY 2009, the total spent by the Department on dental services was $82.8 M. This included $39.6 M in MCO
capitation rates for dental services from January 1, 2009 – June 30, 2009 and $43.2 M for dental services under the
new Maryland Healthy Smiles Dental Program for the period July 1, 2009 – December 31, 2009.
*** Beginning in SFY 2010, Maryland Healthy Smiles Dental Program is reimbursed FFS and paid an
administrative fee. The $6.5 M in CY 2010 and $11.4 M in CY 2011 spent by MCOs account for adult dental
services only and is not reimbursed by the State.
†
The study population for CYs 2008-2015 measured dental utilization for all qualifying individuals in Maryland’s
Medicaid program, including FFS and HealthChoice MCO enrollees. Recipients with partial benefits were excluded
from the analysis.
±
Source: HealthChoice Financial Monitoring Report.
2018 Annual Oral Health Legislative Report
Page 23
Appendix C: State Public Health Dental Programs
County
Local Health
Department Clinic
Community Health
Centers
Dental School/Other
Allegany
On Site
None
Allegany Health Right (contracts
with private dental providers),
Allegany College of Maryland
(Dental Hygiene Program)
Anne
Arundel
On Site (2 sites)
1,2
Baltimore
City
On Site (2 sites)
1,2
Total Health, Chase
Brexton, Park West,
Healthcare for the
Homeless, Family
Health Centers of
Baltimore
University of Maryland School of
Dentistry, University of Maryland
Rehabilitation and Orthopaedic
Institute (formerly Kernan
Hospital), Baltimore City
Community College (Dental
Hygiene Program), University of
Maryland Medical Center
Baltimore
On Site (2 sites)
1
Chase Brexton
Community College of Baltimore
County (Dental Hygiene
Program)
Calvert
None
Calvert Community
Dental Care
Caroline
None
Choptank (2 sites)
Carroll
On Site
None
Access Carroll
3
, Carroll County
Department of Citizen Services
6
Cecil
None
West Cecil Health
Center
University of Maryland School of
Dentistry
Charles
On Site
Served by Calvert
Community Dental
Care
Health Partners
3
Dorchester
None
Choptank
Frederick
On Site
None
Garrett
On Site
None
Harford
On Site
None
Served by University of Maryland
School of Dentistry, Perryville
(Cecil County)
2018 Annual Oral Health Legislative Report
Page 24
County
Local Health
Department Clinic
Community Health
Centers
Dental School/Other
Howard
Subcontract - Chase
Brexton FQHC
Chase Brexton
5
Does not directly provide services
but through its contract with
Chase Brexton FQHC provides
both clinical and school-
based/linked dental services,
Howard County Community
College (Dental Hygiene
Program)
Kent
School-based
program in
partnership with
Queen Anne’s
County Health
Department
Served by Choptank
Served by University of Maryland
School of Dentistry, Perryville
(Cecil County)
Montgomery
On Site (5 sites)
1,5
Community Clinic,
Inc. (CCI)
Prince
George's
On Site (2 sites)
1
Greater Baden, CCI
Fortis College (Dental Hygiene
Program)
Queen
Anne's
School-based
program in
partnership with Kent
County Health
Department
Served by Choptank
Served by University of Maryland
School of Dentistry, Perryville
(Cecil County)
Somerset
None (Served by
Wicomico County
Health Department)
Chesapeake Health
Care
St. Mary's
Serves as an
intermediary between
Medicaid Program
and private dental
providers (Limited
emergency
extraction)
Served by Calvert
Community Dental
Care
Talbot
None
Served by Choptank
Washington
None
Family Healthcare
of Hagerstown
Hagerstown Community College
(Dental Hygiene Program)
Wicomico
On Site
Served by
Chesapeake Health
Care
Worcester
On Site
Served by
Chesapeake Health
Care
2018 Annual Oral Health Legislative Report
Page 25
1 Multiple sites.
2 Began treating Medicaid enrollees in SFY 2013.
3 MCHRC funding beginning in SFY 2010.
4 Partnership between Howard County Health Department and Chase Brexton.
5 Does not currently treat Medicaid enrollees.
6 Discount Dental Program.
2018 Annual Oral Health Legislative Report
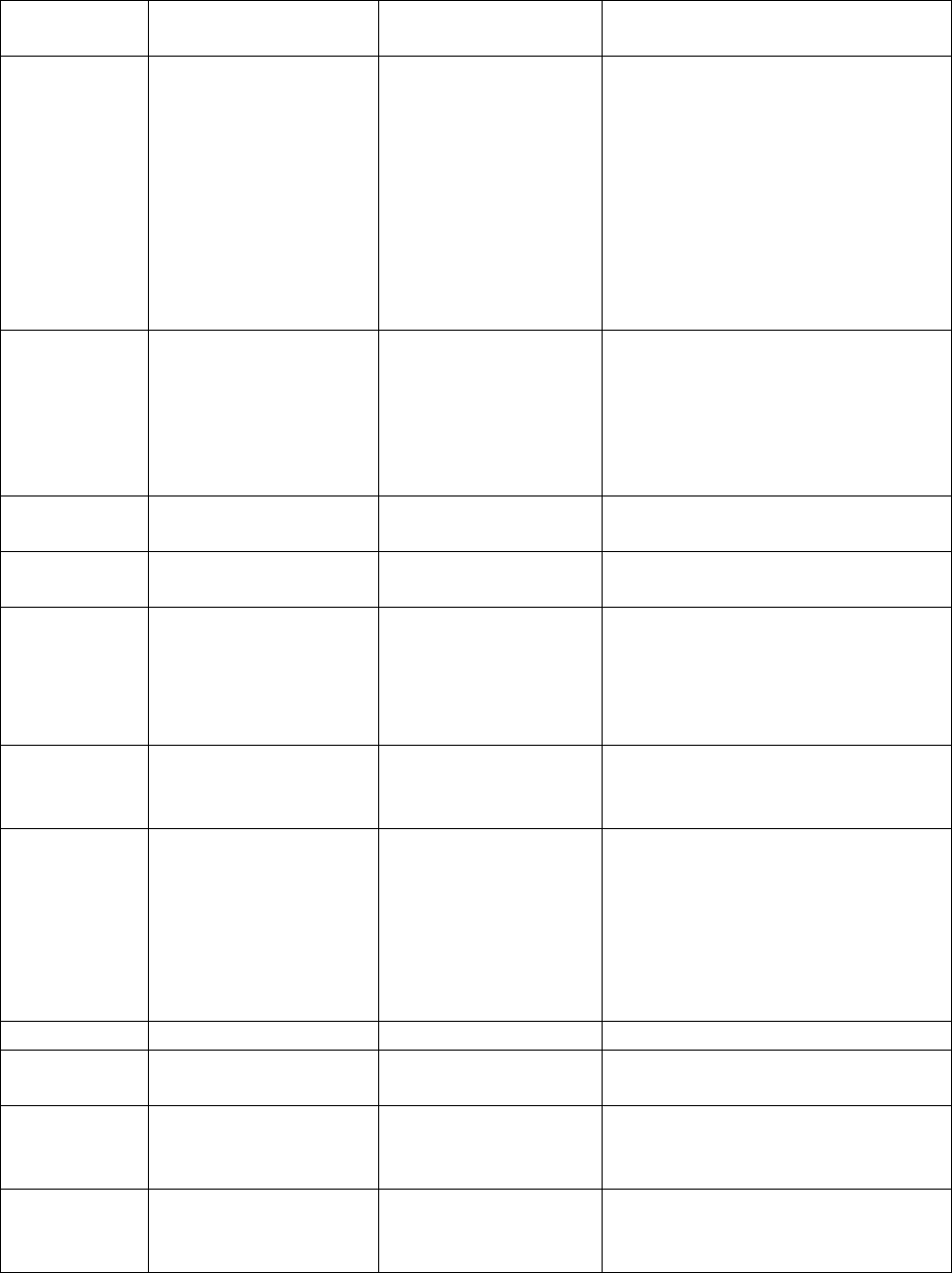
Page 26
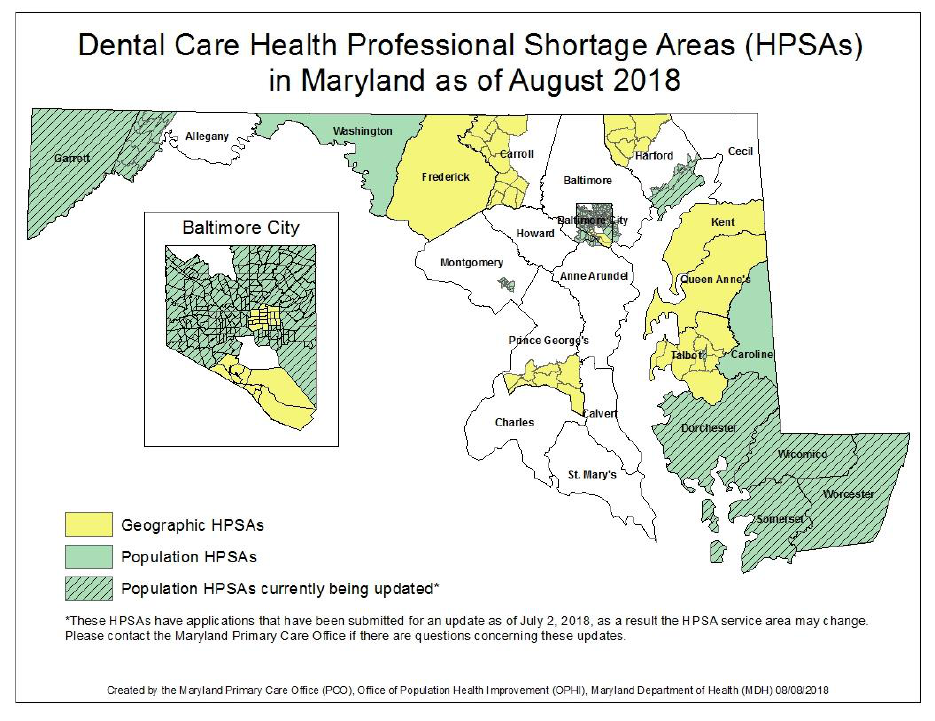
Appendix D: Map of Maryland Health Professional Shortage Areas as of August 2018
2018 Annual Oral Health Legislative Report
Page 27
Appendix E: Medicaid Dental Utilization Rates, CY 2004 – CY 2017 (Enrollment in Medicaid > 320 Days*, Ages 4-20)
Criteria
CY
2004
CY
2005
CY
2006
CY
2007
CY
2008
CY
2009
CY
2010
CY
2011
CY
2012
CY
2013
CY
2014
CY
2015
CY
2016
CY 2017
Age
4-5
43.6%
45.9%
46.2%
52.5%
57.0%
60.9%
67.8%
70.8%
72.3%
72.9%
73.1%
73.9%
73.2%
72.0%
6-9
48.7%
51.1%
51.6%
57.6%
62.5%
65.6%
71.5%
73.8%
74.9%
75.7%
75.2%
76.5%
75.8%
75.0%
10-14
44.8%
46.9%
47.5%
53.2%
57.2%
60.7%
66.4%
68.5%
69.8%
70.0%
69.3%
71.2%
71.2%
71.2%
15-18
37.6%
39.7%
40.2%
44.3%
47.6%
51.2%
55.9%
58.5%
59.4%
59.7%
58.9%
60.3%
60.9%
61.3%
19-20
26.8%
27.7%
26.9%
28.4%
33.2%
37.5%
38.6%
41.2%
43.0%
43.3%
42.7%
43.9%
42.8%
42.9%
All 4-20
43.7%
45.8%
46.2%
51.5%
55.7%
59.0%
63.9%
66.4%
67.8%
68.3%
67.7%
69.0%
68.5%
68.1%
Region**
Baltimore
City
35.8%
38.1%
38.8%
45.9%
51.8%
56.6%
62.4%
64.4%
65.0%
66.2%
65.7%
65.5%
64.6%
64.3%
Baltimore
Suburbs
46.1%
47.0%
47.1%
51.4%
54.8%
56.7%
61.7%
63.6%
66.0%
65.7%
65.6%
66.9%
66.7%
66.4%
Washington
Suburbs
46.4%
50.2%
49.5%
54.8%
58.8%
62.1%
65.8%
70.4%
71.9%
73.3%
72.2%
74.0%
73.6%
73.2%
Western
Maryland
56.1%
56.4%
55.7%
59.3%
61.9%
64.1%
56.9%
69.6%
69.4%
68.2%
67.0%
68.7%
68.0%
67.3%
Southern
Maryland
39.5%
40.0%
43.3%
46.7%
52.2%
56.1%
66.6%
57.5%
58.7%
59.7%
59.7%
59.6%
59.8%
59.1%
Eastern Shore
48.2%
49.2%
51.8%
55.7%
55.7%
59.4%
69.6%
67.9%
69.1%
68.6%
67.5%
69.6%
68.4%
67.7%
All Regions
43.7%
45.8%
46.2%
51.5%
55.7%
59.0%
63.9%
66.4%
67.8%
68.3%
67.7%
69.0%
68.5%
68.1%
*
The study population for CY 2014 measured dental utilization for all qualifying individuals in Medicaid, including FFS and HealthChoice MCO enrollees. The
following coverage groups were excluded from the analysis: S09, X02, W01, and P10.
**
Baltimore Suburbs includes Anne Arundel, Baltimore, Carroll, Harford, and Howard Counties. Washington, D.C. suburbs include Prince George’s and
Montgomery Counties. Southern Maryland includes Calvert, Charles, and St. Mary’s Counties. Western Maryland includes Allegany, Frederick, Garrett, and
Washington Counties. The Eastern Shore includes Caroline, Cecil, Dorchester, Kent, Queen Anne’s, Somerset, Talbot, Wicomico, and Worcester Counties.
